Welcome students and residents to the Pediatric Cardiology Multiple Choice Questions. Please make every effort to complete all questions during your first rotation week, review the answers/explanations and take the test again in the last week of your rotation. By doing that you’ll be able to assess your own performance. For us, we’ll be able to modify the rotation outline based on your test result. The system will save your answers if you want to take the test on multiple sessions.
Time limit: 0
Quiz-summary
0 of 39 questions completed
Questions:
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
Information
CCHD Exam – Part I
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You must sign in or sign up to start the quiz.
You have to finish following quiz, to start this quiz:
Results
0 of 39 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 points, (0)
Average score
Your score
Categories
Cardiovascular physiology, anatomy and pathology0%
History in children with heart disease0%
Physical examination in children with heart disease0%
Congratulations on a job well done!
Your result has been entered into leaderboard
Loading
maximum of 42 points
Pos.
Name
Entered on
Points
Result
Table is loading
No data available
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
Answered
Review
Question 1 of 39
1. Question
1 points
Category: Cardiovascular physiology, anatomy and pathology
A 6 month old girl, known to have large ventricular septal defect initially gained weight appropriately, however, 2 months ago began to gain weight poorly, and in the last 2 weeks is loosing weight. The child is on digoxin, lasix and captopril. The cause of weight loss in this child could be attributed to:
Correct
That is Correct!
Children with large ventricular septal defects develop large left to right shunting and increased pulmonary blood flow. This will result in pulmonary edema, producing difficulty in breathing effort (tachypnea and respiratory distress). The left to right shunting at the septal defect causes volume overload of the right ventricle and the increase in pulmonary blood flow will cause the pulmonary venous return to increase thus overloading the left heart as well. This increase in cardiac load will cause myocardial fatigue.
The increase in work load of the myocardium and respiratory system consumes a significant portion of caloric intake, which together with reduced caloric intake due to respiratory distress and inability to feed properly will lead to failure to thrive.
Option B is incorrect since these medications do not interfere with intestinal absorption.
Option C is incorrect since pulmonary stenosis would actually restrict pulmonary blood flow resulting in less and not more congestive heart failure.
Option D is incorrect, since elevation in pulmonary vascular resistance, though carries worse prognosis, actually causes less pulmonary blood flow and consequently less congestive heart failure.
Incorrect
Correct answer is A:
Children with large ventricular septal defects develop large left to right shunting and increased pulmonary blood flow. This will result in pulmonary edema, producing difficulty in breathing effort (tachypnea and respiratory distress). The left to right shunting at the septal defect causes volume overload of the right ventricle and the increase in pulmonary blood flow will cause the pulmonary venous return to increase thus overloading the left heart as well. This increase in cardiac load will cause myocardial fatigue.
The increase in work load of the myocardium and respiratory system consumes a significant portion of caloric intake, which together with reduced caloric intake due to respiratory distress and inability to feed properly will lead to failure to thrive.
Option B is incorrect since these medications do not interfere with intestinal absorption.
Option C is incorrect since pulmonary stenosis would actually restrict pulmonary blood flow resulting in less and not more congestive heart failure.
Option D is incorrect, since elevation in pulmonary vascular resistance, though carries worse prognosis, actually causes less pulmonary blood flow and consequently less congestive heart failure.
Question 2 of 39
2. Question
1 points
Category: History in children with heart disease
A one week old is seen at well child care. Mom is concerned that the baby is not feeding well. He takes one half to one ounce every 1-2 hours, thereafter he falls asleep. HR 70 bpm, RR is 45/min; Examination reveals no cyanosis or jaundice. A wide spread rash is noted over the face and trunk. Capillary refill is 3 seconds. Femoral and brachial arterial pulses are equal and full. Liver edge is palpated at 4-5 cm below right costal margin. Lungs are clear to auscultation, S1 is normal; S2 splits with no systolic or diastolic murmurs.
Important question to ask mother is:
Correct
That is Correct!
This child has a heart rate of 75 bpm, which is slow for this age. This may be a manifestation of fetal affliction by maternal systemic lupus erythematosus. Electrocardiography will most probably show complete atrioventricular block. The poor feeding, hepatomegaly and delayed capillary refill (normal less than 2 seconds) are all features of poor cardiac output and heart failure secondary to bradycardia. The rash is another manifestation of systemic lupus erythematosus. Other cardiac complications of maternal lupus include cardiomyopathy and l-transposition of the great vessels, also known as ventricular inversion or corrected transposition.
Option A is incorrect since the type of formula is irrelevant when the problem is small volume of feeds. Babies may poorly tolerate certain formulas resulting in emesis or diarrhea.
Option B is incorrect since nursing is irrelevant in this case, particularly with clear symptoms of heart failure.
Option D is incorrect since auscultation does not appear to suggest congenital heart disease, but instead the problem seems to stem from a slow heart rate.
Incorrect
Correct answer is C:
This child has a heart rate of 75 bpm, which is slow for this age. This may be a manifestation of fetal affliction by maternal systemic lupus erythematosus. Electrocardiography will most probably show complete atrioventricular block. The poor feeding, hepatomegaly and delayed capillary refill (normal less than 2 seconds) are all features of poor cardiac output and heart failure secondary to bradycardia. The rash is another manifestation of systemic lupus erythematosus. Other cardiac complications of maternal lupus include cardiomyopathy and l-transposition of the great vessels, also known as ventricular inversion or corrected transposition.
Option A is incorrect since the type of formula is irrelevant when the problem is small volume of feeds. Babies may poorly tolerate certain formulas resulting in emesis or diarrhea.
Option B is incorrect since nursing is irrelevant in this case, particularly with clear symptoms of heart failure.
Option D is incorrect since auscultation does not appear to suggest congenital heart disease, but instead the problem seems to stem from a slow heart rate.
Question 3 of 39
3. Question
1 points
Category: History in children with heart disease
A 13 year old girl weighs 35 kg and is 178 cm tall. She is asymptomatic and is seen for assessment of a heart murmur detected by school nurse. Heart rate is 80 bpm, respiratory rate is 20/min. BP in right arm is 110/70. Mucosa is pink, capillary refill is brisk. Femoral and arterial pulses are equal and full. No hepatomegaly is detected. Precordium is with no palpable thrill. On auscultation, first heart sound is normal, second heart sound splits and varies with respiration. There is a 3/6 holosystolic murmur at apex. System review shows significant myopia. Family history is not significant.
In addition to mitral regurgitation, what else would you expect the echocardiogram to demonstrate?
Correct
That is Correct!
This child appears to have Marfan syndrome, an autosomal dominant disease which may present as a spontaneous mutation with negative family history. This child is tall (above 95 percentile) with myopia and a murmur consistent with mitral regurgitation. Patients with Marfan syndrome are tall, with long arm length span and ocular abnormalities such as myopia and retinal detachment. The cardiac pathologies, which are secondary to collagen disorder, present as mitral valve prolapse, mitral regurgitation, aortic root dilation and aortic regurgitation. Patients with Marfan syndrome may develop significant aortic root dilation, leading to aneurysm and aortic root rupture with catastrophic consequences.
Option A is incorrect since the murmur is consistent with mitral regurgitation and not ventricular septal defect (VSD). VSD murmurs are heard best at the left lower sternal border.
Option C is incorrect since a murmur of aortic stenosis is heard as a harsh ejection systolic murmur at right upper sternal border. Patients with Marfan syndrome are not at risk to develop aortic stenosis.
Option D is incorrect since the murmur is not consistent with tricuspid valve regurgitation.
Incorrect
Correct answer is B:
This child appears to have Marfan syndrome, an autosomal dominant disease which may present as a spontaneous mutation with negative family history. This child is tall (above 95 percentile) with myopia and a murmur consistent with mitral regurgitation. Patients with Marfan syndrome are tall, with long arm length span and ocular abnormalities such as myopia and retinal detachment. The cardiac pathologies, which are secondary to collagen disorder, present as mitral valve prolapse, mitral regurgitation, aortic root dilation and aortic regurgitation. Patients with Marfan syndrome may develop significant aortic root dilation, leading to aneurysm and aortic root rupture with catastrophic consequences.
Option A is incorrect since the murmur is consistent with mitral regurgitation and not ventricular septal defect (VSD). VSD murmurs are heard best at the left lower sternal border.
Option C is incorrect since a murmur of aortic stenosis is heard as a harsh ejection systolic murmur at right upper sternal border. Patients with Marfan syndrome are not at risk to develop aortic stenosis.
Option D is incorrect since the murmur is not consistent with tricuspid valve regurgitation.
Question 4 of 39
4. Question
1 points
Category: History in children with heart disease
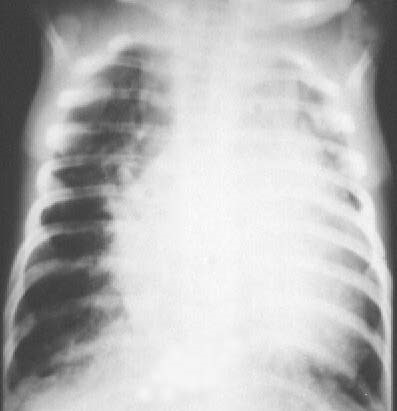
A 3 month old infant, born at 29 weeks gestation, in the neonatal intensive care unit continues to require ventilatory support due to severe and chronic lung disease attributed to prematurity. A recent short and harsh ejection systolic murmur is heard over the left mid-sternal border. Vital signs and physical examination is otherwise unchanged. Echocardiography demonstrates severe, bilateral ventricular hypertrophy with intracavitory obstruction to flow within the right and left ventricles.
The cardiac changes could be attributed to:
Correct
That is Correct!
Steroids used chronically in premature infants in the treatment of chronic lung disease due to prematurity may cause hypertrophic cardiomyopathy. This resolves when steroid therapy is withdrawn. Hypertrophied muscles will cause reduction of ventricular cavity size leading to obstruction to blood flow.
Option A and C are incorrect since these are not known side effects to these medications.
Option D is incorrect since core pulmonale may cause right ventricular hypertrophy and right heart failure, however, the left heart will not be affected.
Incorrect
Correct answer is B:
Steroids used chronically in premature infants in the treatment of chronic lung disease due to prematurity may cause hypertrophic cardiomyopathy. This resolves when steroid therapy is withdrawn. Hypertrophied muscles will cause reduction of ventricular cavity size leading to obstruction to blood flow.
Option A and C are incorrect since these are not known side effects to these medications.
Option D is incorrect since core pulmonale may cause right ventricular hypertrophy and right heart failure, however, the left heart will not be affected.
Question 5 of 39
5. Question
1 points
Category: History in children with heart disease
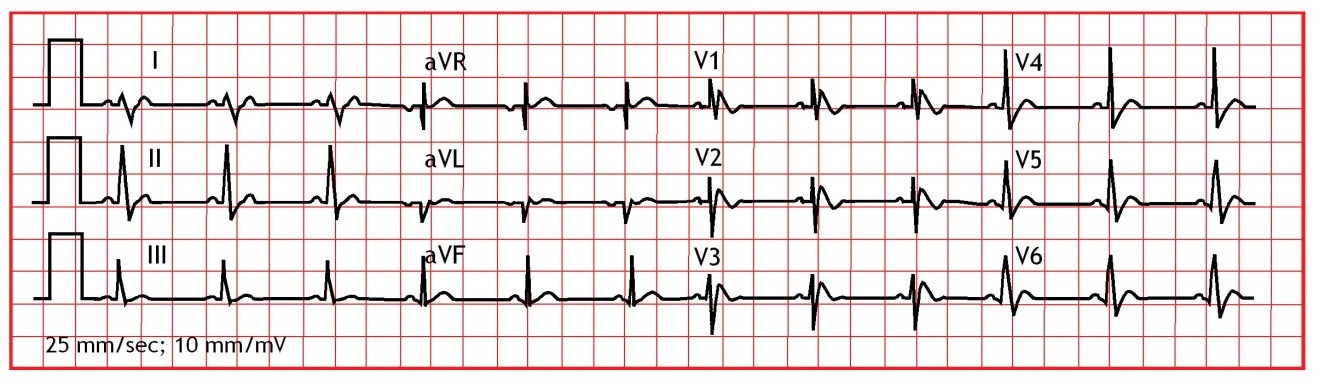
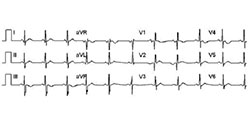
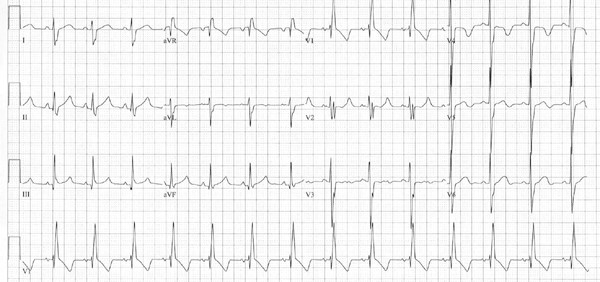
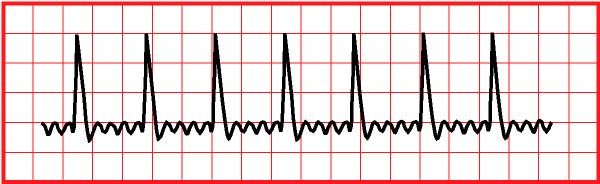
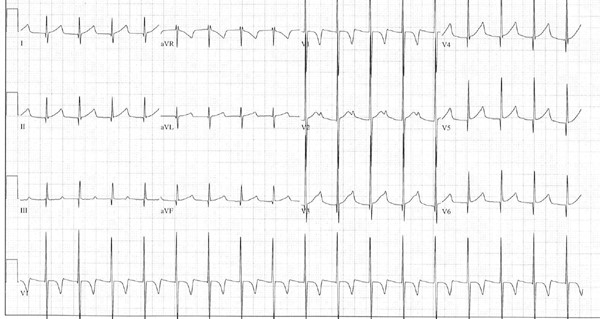
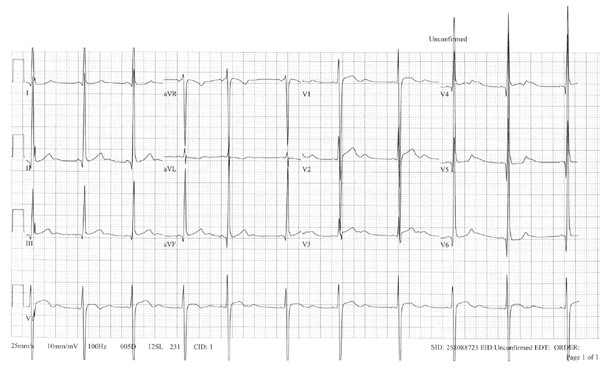
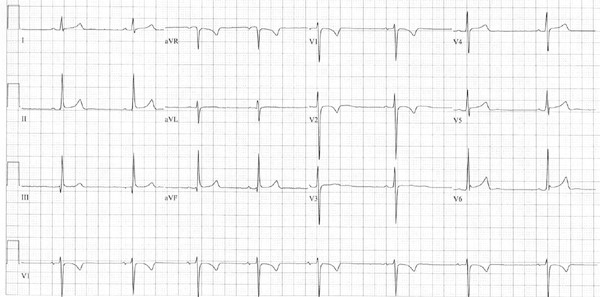
A 4 year old child is referred to the emergency room for evaluation of abnormal heart rate. The child was seen in the pediatrician’s office for evaluation of emesis when a heart rate of 60 bpm was detected. The child has had a viral URI for few days but was thought to be getting better when emesis developed overnight. Past medical history is unremarkable; the child was receiving a decongestant-cold medication for the past 2 days. Family history is remarkable for a grandmother who resides with the child who suffers from congestive heart failure and history of tachyarrhythmia.
12 lead ECG and rhythm strip is shown below.
Correct
That is Correct!
This child has sinus bradycardia with first degree atrioventricular block (AVB). The cold symptoms do not appear to be related to bradycardia. Fever, due to a viral infection causes sinus tachycardia, not bradycardia. Cold medications with decongestants cause tachycardia as well. Congestive heart failure may be treated with digoxin which if ingested inadvertently by a toddler may cause bradycardia and first degree AVB. Management of a child with digoxin toxicity may include Digibind; this is used when the total ingested dose is > 4 mg in children or > 10 mg in adults. It is also used if there are significant ECG changes, such as ventricular arrhythmias. First degree AVB and mild sinus bradycardia could be observed. Hyperkalemia results from digoxin toxicity, not Hypokalemia. Emesis induction or activated charcoal is used when ingestion is less than 30 minutes ago.
Incorrect
Correct answer is C:
This child has sinus bradycardia with first degree atrioventricular block (AVB). The cold symptoms do not appear to be related to bradycardia. Fever, due to a viral infection causes sinus tachycardia, not bradycardia. Cold medications with decongestants cause tachycardia as well. Congestive heart failure may be treated with digoxin which if ingested inadvertently by a toddler may cause bradycardia and first degree AVB. Management of a child with digoxin toxicity may include Digibind; this is used when the total ingested dose is > 4 mg in children or > 10 mg in adults. It is also used if there are significant ECG changes, such as ventricular arrhythmias. First degree AVB and mild sinus bradycardia could be observed. Hyperkalemia results from digoxin toxicity, not Hypokalemia. Emesis induction or activated charcoal is used when ingestion is less than 30 minutes ago.
Question 6 of 39
6. Question
1 points
Category: History in children with heart disease
An 8 year old girl followed by a GI specialist for the past few years for irritable bowel disease. She was referred to a pediatric cardiologist for evaluation of a heart murmur. Heart rate 90 bpm, respiratory rate 20/minute, Oxygen saturation 95% while breathing room air, BP in right upper extremity 110/60 mmHg. Mucosa is pink, though pale. Capillary refill is brisk. Fingers show clubbing. No hepatomegaly is present, precordium is hyperactive with increase right and left ventricular impulse, no palpable thrill. The murmur is 2/6 systolic flow murmur heard over the left and right upper sternal borders. Lungs were clear to auscultation bilaterally. The cardiologist felt that the heart murmur is secondary to increase flow across aortic and pulmonary valves due to chronic anemia.
What is the most probable cause of clubbing of fingers in this patient?
Correct
That is Correct!
Irritable bowl disease causes chronic anemia, which results in chronic hypoxia, which like cyanotic heart disease and chronic lung disease may lead to clubbing of fingers. This patient has no evidence of significant heart or lung disease. Idiopathic clubbing is possible, though rare.
Clubbing of fingers resulting from hypoxia which induces tissues to expand capillary beds to increase blood flow, this will result in thickening of peripheral tissues, such as fingers and toes.
Incorrect
Correct answer is A:
Irritable bowl disease causes chronic anemia, which results in chronic hypoxia, which like cyanotic heart disease and chronic lung disease may lead to clubbing of fingers. This patient has no evidence of significant heart or lung disease. Idiopathic clubbing is possible, though rare.
Clubbing of fingers resulting from hypoxia which induces tissues to expand capillary beds to increase blood flow, this will result in thickening of peripheral tissues, such as fingers and toes.
Question 7 of 39
7. Question
1 points
Category: Cardiovascular physiology, anatomy and pathology
A one year old girl presents with failure to thrive. The child is eager to feed, however, after one ounce develops shortness of breath, pallor and sweating. Mom notes that her extremities become cool and mottled after feeding. Physical examination is remarkable for an undernourished child with tachypnea, nasal flaring and intercostals as well as subcostal retractions. HR is 150 bpm, RR is 60/min, BP is 110/40 mmHg, O2 saturation is 95%. Liver is enlarged and LV apical impulse is increased. 3/6 continuous murmur is heard over the left subclavicular region. Echocardiography shows large patent ductus arteriosus. Pulmonary arterial systolic pressure as assessed through tricuspid regurgitation jet was 110 mmHg.
The systemic pulmonary arterial pressure indicates that:
Correct
Patients with increased pulmonary blood flow due to a shunt at the atrial, ventricular or great vessel levels will develop pulmonary hypertension due to increased pulmonary blood flow. Pulmonary arterial pressure (P) is a product of flow (Q) and resistance (R):
P = Q X R
Elevated pressure can be produced by elevation in flow rate or vascular resistance. In the case scenario presented here the child has symptoms of congestive heart failure due to increased pulmonary blood flow. This means that the pulmonary vascular resistance must be low to allow for this increased pulmonary blood flow.
Furthermore, the natural history of PDA is that patients do not develop elevation of pulmonary vascular resistance in the first decade of life.
Option A is incorrect because it does not make the distinction between elevated pulmonary arterial pressure due to high flow or high pulmonary vascular resistance. The former seems to be the case here. Therefore, pulmonary arterial pressure will be reduced once the increased pulmonary blood flow is eliminated through PDA closure.
Option B is also incorrect since this is a false statement. PDA should not be closed if pulmonary vascular resistance is elevated, since this will not be helped by ductal closure and it is even dangerous since the PDA serves as a pop off for elevated right heart pressure. Acute right heart failure will result if PDA is closed in view of elevated pulmonary vascular resistance.
Option D is incorrect since method of closure does is not dictated by pulmonary vascular resistance. Both methods of treatment are dictated by the same principals. Method of closure is dictated by size of PDA and age of patient.
Incorrect
Answer is C
Patients with increased pulmonary blood flow due to a shunt at the atrial, ventricular or great vessel levels will develop pulmonary hypertension due to increased pulmonary blood flow. Pulmonary arterial pressure (P) is a product of flow (Q) and resistance (R):
P = Q X R
Elevated pressure can be produced by elevation in flow rate or vascular resistance. In the case scenario presented here the child has symptoms of congestive heart failure due to increased pulmonary blood flow. This means that the pulmonary vascular resistance must be low to allow for this increased pulmonary blood flow.
Furthermore, the natural history of PDA is that patients do not develop elevation of pulmonary vascular resistance in the first decade of life.
Option A is incorrect because it does not make the distinction between elevated pulmonary arterial pressure due to high flow or high pulmonary vascular resistance. The former seems to be the case here. Therefore, pulmonary arterial pressure will be reduced once the increased pulmonary blood flow is eliminated through PDA closure.
Option B is also incorrect since this is a false statement. PDA should not be closed if pulmonary vascular resistance is elevated, since this will not be helped by ductal closure and it is even dangerous since the PDA serves as a pop off for elevated right heart pressure. Acute right heart failure will result if PDA is closed in view of elevated pulmonary vascular resistance.
Option D is incorrect since method of closure does is not dictated by pulmonary vascular resistance. Both methods of treatment are dictated by the same principals. Method of closure is dictated by size of PDA and age of patient.
Question 8 of 39
8. Question
1 points
Category: Cardiovascular physiology, anatomy and pathology
While examining a patient with L-TGA (corrected transposition of the great vessels) the single second heart sound appears to be single without splitting, there are no associated murmurs. This could be attributed to which one of the following:
Correct
That is Correct!
In corrected transposition the two ventricles are inverted, thus the left atrium leads to an anatomical right ventricle which functions as the systemic ventricle. This ventricle leads to an anterior aortic valve (normally the aortic valve is posterior). The right atrium on the other hand leads to an anatomical left ventricle which functions as the pulmonary ventricle. This ventricle leads to a posterior pulmonary valve. This switch in position of semilunar valves will cause the typically soft sound of the pulmonary valve closure to be inaudible as it is posterior to the aortic valve and far away from the chest wall.
Option A is incorrect, since it is never normal to have a single heart sound throughout the respiratory cycle. Second heart sound is caused by closure of the pulmonary and aortic valve. The pulmonary valve closes after the aortic valve since the left ventricle, due to shorter left bundle branch contracts few milliseconds before the right ventricle and therefore finishes contraction earlier than the right ventricle. This causes the aortic valve to close just before the pulmonary valve, this becomes evident during inspiration when the pulmonary valve stays open even later than usual to deal with the increase blood volume in the right ventricle due to the effect of the negative intrathoracic pressure in inspiration due to chest expansion which acts as a sump effect to increase blood return to the heart. Second heart sound is single only during expiratory phase of respiration when the two valves closures become too close to differentiate as two components. This is caused by the reduced blood return (pre-load) to the heart during expiratory phase due to increased intrathoracic pressure during expiration.
Option C is incorrect. It is true that significant pulmonary or aortic stenosis will cause the single heart sound to be single due to the deformity of the affected valve and lack of normal motion of that valve. However, in this case there is no systolic murmur, which must be associated with severe pulmonary or aortic valve stenosis.
Option D is incorrect since pulmonary hypertension will actually cause the pulmonary valve to close with greater force resulting in a louder pulmonary component of the second heart sound, not softer.
Incorrect
Correct answer is B:
In corrected transposition the two ventricles are inverted, thus the left atrium leads to an anatomical right ventricle which functions as the systemic ventricle. This ventricle leads to an anterior aortic valve (normally the aortic valve is posterior). The right atrium on the other hand leads to an anatomical left ventricle which functions as the pulmonary ventricle. This ventricle leads to a posterior pulmonary valve. This switch in position of semilunar valves will cause the typically soft sound of the pulmonary valve closure to be inaudible as it is posterior to the aortic valve and far away from the chest wall.
Option A is incorrect, since it is never normal to have a single heart sound throughout the respiratory cycle. Second heart sound is caused by closure of the pulmonary and aortic valve. The pulmonary valve closes after the aortic valve since the left ventricle, due to shorter left bundle branch contracts few milliseconds before the right ventricle and therefore finishes contraction earlier than the right ventricle. This causes the aortic valve to close just before the pulmonary valve, this becomes evident during inspiration when the pulmonary valve stays open even later than usual to deal with the increase blood volume in the right ventricle due to the effect of the negative intrathoracic pressure in inspiration due to chest expansion which acts as a sump effect to increase blood return to the heart. Second heart sound is single only during expiratory phase of respiration when the two valves closures become too close to differentiate as two components. This is caused by the reduced blood return (pre-load) to the heart during expiratory phase due to increased intrathoracic pressure during expiration.
Option C is incorrect. It is true that significant pulmonary or aortic stenosis will cause the single heart sound to be single due to the deformity of the affected valve and lack of normal motion of that valve. However, in this case there is no systolic murmur, which must be associated with severe pulmonary or aortic valve stenosis.
Option D is incorrect since pulmonary hypertension will actually cause the pulmonary valve to close with greater force resulting in a louder pulmonary component of the second heart sound, not softer.
Question 9 of 39
9. Question
1 points
Category: Cardiovascular physiology, anatomy and pathology
Patients with large atrial and ventricular septal defects as well as large patent ductus arteriosus exhibit symptoms of congestive heart failure for the first 2-3 decades of life, thereafter, these patients may show resolution of these symptoms, despite echocardiographic evidence of persistence of large defects. This could be explained by which of the following mechanisms:
Correct
That is Correct!
The extent of shunting across any communication between the right and left heart is determined by the resistance facing blood in either direction. Blood in the left ventricle, in the case of ventricular septal defect (VSD) can flow through the aortic valve and out into the systemic circulation, as it normally does, facing a systemic vascular resistance of about 25 Wood units (mmHg/L/min/M2). Or cross the VSD and flow towards the pulmonary vascular bed, facing the resistance offered by the size of the VSD itself and the pulmonary vascular resistance, typically 1-3 Wood units. If the VSD is large enough it will not cause any resistance and the only determinant of blood flow across the VSD becomes the difference between the systemic and pulmonary vascular resistance, the higher the systemic vascular resistance and lower the pulmonary vascular resistance, the larger is the volume of shunting. The opposite is also true. This is based on the physics principal of that fluid will flow to where resistance is least.
Option B is incorrect as it is opposite to the above stated theory.
Option C is incorrect since over time the right ventricle over time develops pathological changes, including fibrosis.
Option D is incorrect since the pulmonary vasculature of time develops vascular changes. Initially, these changes are reversible, but eventually become permanent. Damage to pulmonary vasculature causes the pulmonary vascular resistance to increase, and thus reduce pulmonary blood flow. Therefore the compliance of the pulmonary blood vessels decreases and not increases overtime.
Incorrect
Correct answer is A
The extent of shunting across any communication between the right and left heart is determined by the resistance facing blood in either direction. Blood in the left ventricle, in the case of ventricular septal defect (VSD) can flow through the aortic valve and out into the systemic circulation, as it normally does, facing a systemic vascular resistance of about 25 Wood units (mmHg/L/min/M2). Or cross the VSD and flow towards the pulmonary vascular bed, facing the resistance offered by the size of the VSD itself and the pulmonary vascular resistance, typically 1-3 Wood units. If the VSD is large enough it will not cause any resistance and the only determinant of blood flow across the VSD becomes the difference between the systemic and pulmonary vascular resistance, the higher the systemic vascular resistance and lower the pulmonary vascular resistance, the larger is the volume of shunting. The opposite is also true. This is based on the physics principal of that fluid will flow to where resistance is least.
Option B is incorrect as it is opposite to the above stated theory.
Option C is incorrect since over time the right ventricle over time develops pathological changes, including fibrosis.
Option D is incorrect since the pulmonary vasculature of time develops vascular changes. Initially, these changes are reversible, but eventually become permanent. Damage to pulmonary vasculature causes the pulmonary vascular resistance to increase, and thus reduce pulmonary blood flow. Therefore the compliance of the pulmonary blood vessels decreases and not increases overtime.
Question 10 of 39
10. Question
1 points
Category: Cardiovascular physiology, anatomy and pathology
A patient with pulmonary stenosis develops a harsh systolic ejection murmur over the left upper sternal border, though the pulmonary valve originates from the right ventricle. On the other hand, a patient with aortic stenosis develops a similar murmur over the right upper sternal border, though the aortic valve originates from the left ventricle. The cause of this apparent discrepancy between the origin of the semilunar valve and the location at which its pathology is heard is due to:
Correct
That is Correct!
The right and left ventricle is anterior and to the right of the left ventricle, while the left ventricle is posterior and to the left of the right ventricle. The outflow tracts of each ventricle crisscross each other to deliver the semilunar valves at the opposite side of the chest of their respective ventricle. This renders the aortic valve to the right of the pulmonary valve.
Option A is incorrect since heart murmurs may travel in the direction of blood flow giving a “referred” sound; however, they will always be heard at their original location as well.
Option B is incorrect since involvement of the other semilunar valve, though rare, will cause murmurs at both right upper and left upper sternal borders.
Option C is incorrect. It is true that chest wall is thin in children causing auscultation to be easier and heart sounds to be heard outside the area over the chest closest to the affected valve, however, the loudest sound remains at the location of affected valve, i.e. left upper chest in pulmonary valve disease and right upper chest in aortic valve disease.
Incorrect
Correct answer is D
The right and left ventricle is anterior and to the right of the left ventricle, while the left ventricle is posterior and to the left of the right ventricle. The outflow tracts of each ventricle crisscross each other to deliver the semilunar valves at the opposite side of the chest of their respective ventricle. This renders the aortic valve to the right of the pulmonary valve.
Option A is incorrect since heart murmurs may travel in the direction of blood flow giving a “referred” sound; however, they will always be heard at their original location as well.
Option B is incorrect since involvement of the other semilunar valve, though rare, will cause murmurs at both right upper and left upper sternal borders.
Option C is incorrect. It is true that chest wall is thin in children causing auscultation to be easier and heart sounds to be heard outside the area over the chest closest to the affected valve, however, the loudest sound remains at the location of affected valve, i.e. left upper chest in pulmonary valve disease and right upper chest in aortic valve disease.
Question 11 of 39
11. Question
1 points
Category: Cardiovascular physiology, anatomy and pathology
Clubbing of digits in a 14 year old boy with cyanotic congenital heart disease is a reflection of which one of the following pathophysiologic factors?
Correct
That is Correct!
Patients with cyanosis have lower oxygen blood content, resulting in tissue hypoxia. In compensation, peripheral tissue which is most deprived of oxygen, such as the digits will increase capillary bed capacity to enable tissue to extract more oxygen. The expansion in capillary bed capacity will result in an increase in tissue mass, manifested as clubbing.
Option A is incorrect since PaCO2 does not increase in cyanosis. PaCo2 is a reflection of respiratory status.
Option B is incorrect since Heart rate has no bearing on tissue perfusion unless it is extremely rapid, as in tachyarrhythmias or extremely slow.
Option C is incorrect since congestive heart failure typically causes peripheral edema rather than clubbing.
Incorrect
Correct answer is D
Patients with cyanosis have lower oxygen blood content, resulting in tissue hypoxia. In compensation, peripheral tissue which is most deprived of oxygen, such as the digits will increase capillary bed capacity to enable tissue to extract more oxygen. The expansion in capillary bed capacity will result in an increase in tissue mass, manifested as clubbing.
Option A is incorrect since PaCO2 does not increase in cyanosis. PaCo2 is a reflection of respiratory status.
Option B is incorrect since Heart rate has no bearing on tissue perfusion unless it is extremely rapid, as in tachyarrhythmias or extremely slow.
Option C is incorrect since congestive heart failure typically causes peripheral edema rather than clubbing.
Question 12 of 39
12. Question
1 points
Category: Cardiovascular physiology, anatomy and pathology
Which one of the following case scenarios with pericardial effusion would be least likely to deteriorate hemodynamically?
Correct
That is Correct!
Children with Down syndrome may develop lymphatic pericardial effusion which may reach large volume without symptoms or signs of cardiac tamponade due to slow accumulation.
Option A is incorrect since large pericardial effusion in this patient represents post-pericardiotomy syndrome which if large may cause hemodynamic instability.
Option C is incorrect since this patient seems to have purulent pericardial effusion secondary to mediastinitis. These patients tend to be very ill.
Option D is incorrect since this child appears to have post-operative bleeding which may cause acute deterioration of patient and will require possible surgical intervention.
Incorrect
Correct answer is B:
Children with Down syndrome may develop lymphatic pericardial effusion which may reach large volume without symptoms or signs of cardiac tamponade due to slow accumulation.
Option A is incorrect since large pericardial effusion in this patient represents post-pericardiotomy syndrome which if large may cause hemodynamic instability.
Option C is incorrect since this patient seems to have purulent pericardial effusion secondary to mediastinitis. These patients tend to be very ill.
Option D is incorrect since this child appears to have post-operative bleeding which may cause acute deterioration of patient and will require possible surgical intervention.
Question 13 of 39
13. Question
1 points
Category: History in children with heart disease
A mother is concerned that her 2 day old has bluish discoloration of the skin. She has researched this issue on the internet and is concerned that the child may have congenital heart disease. The baby was born at full term; pregnancy was complicated with maternal diabetes. Baby feeds 3 ounces of formula every 3 hours. Mom denies any shortness of breath. On examination the child is alert, there is no respiratory distress. There is bluish discoloration of the legs and feet with some mottling complexion of arms and legs. The oral mucosa is pink. HR is 130 bpm, regular, RR is 30/min. Capillary refill is 2 seconds in feet and hands. There is no hepatomegaly. No palpable thrill is elicited. First heart sound is single, second heart sound splits and varies throughout respiration. A 2/6 soft systolic murmur is heard over the left upper sternal border with radiation to left axilla.
Correct statement regarding the cyanosis in this patient is:
Correct
That is Correct!
This child appears to have acrocyanosis, a normal finding of this age group. Acrocyanosis in the neonatal period is due to immaturity of the peripheral vasculature. It does not reflect any congenital heart disease since the more richly supplied tissue, such as oral mucosa appears well oxygenated. The murmur in this child is typical of peripheral pulmonary stenosis, a normal finding in neonates.
Option A is incorrect since the cyanosis is peripheral (acrocyanosis) and not central cyanosis as seen in tetralogy of Fallot.
Option C is incorrect since the murmur is soft and most probably due to peripheral pulmonary stenosis, a normal finding at this age group.
Option D is incorrect since all findings are within normal limits and not indicative of any congenital heart disease. Infants of children with diabetic mothers are likely to develop hypertrophic cardiomyopathy. These babies are more likely than the general population to have transposition of the great arteries, ventricular septal defect or coarctation of the aorta, though the incidence of these defects is still low.
Incorrect
Correct answer is B:
This child appears to have acrocyanosis, a normal finding of this age group. Acrocyanosis in the neonatal period is due to immaturity of the peripheral vasculature. It does not reflect any congenital heart disease since the more richly supplied tissue, such as oral mucosa appears well oxygenated. The murmur in this child is typical of peripheral pulmonary stenosis, a normal finding in neonates.
Option A is incorrect since the cyanosis is peripheral (acrocyanosis) and not central cyanosis as seen in tetralogy of Fallot.
Option C is incorrect since the murmur is soft and most probably due to peripheral pulmonary stenosis, a normal finding at this age group.
Option D is incorrect since all findings are within normal limits and not indicative of any congenital heart disease. Infants of children with diabetic mothers are likely to develop hypertrophic cardiomyopathy. These babies are more likely than the general population to have transposition of the great arteries, ventricular septal defect or coarctation of the aorta, though the incidence of these defects is still low.
Question 14 of 39
14. Question
1 points
Category: History in children with heart disease
A 6 year old girl with large PDA is described by her parents to have easy fatigability. She tends to tire easy when playing with children her age requiring her to sit down and rest. She is accustomed to having at least one nap a day. The family lives in a second floor apartment. The child has to rest half way as she ascends the stairs to the apartment. These symptoms of easy fatigability clearly reflect congestive heart failure. How would the parents describe easy fatigability if this child was an infant rather than a 6 year old?
Correct
That is Correct!
Easy fatigability in infants with congestive heart failure is manifested by inability to feed for the usual period of time due to lack of energy to sustain this effort. This is caused by reduced caloric intake, increased caloric expenditure by the respiratory system and myocardium as well as inability to increase the respiratory work since it is already at maximum capacity due to pulmonary edema.
Option B is incorrect since sucking during feeding in infants is significant exercise effort.
Option C is incorrect. Shortness of breath does occur in congestive heart failure, though this id due to pulmonary edema which decreases the gaseous exchange as the fluid in the pulmonary tissue accumulates. Pulmonary edema also makes the lungs less distensible, requiring the use of intercostals muscles to assist in breathing. Respiratory distress is a cause for easy fatigability as it is an effort to perform, but it is not a manifestation of it.
Option D is incorrect. Cyanosis occurs due to obligatory right to left shunting within th heart, such as with tricuspid atresia. This is not a manifestation of easy fatigability, rather it reflects the presence of a communication between the right heart and the left heart and the inability of deoxygenated blood in the right heart to proceed to the lungs to get oxygenated, and instead being diverted to the left heart to mix with well oxygenated blood, thus causing cyanosis.
Incorrect
Correct answer is A
Easy fatigability in infants with congestive heart failure is manifested by inability to feed for the usual period of time due to lack of energy to sustain this effort. This is caused by reduced caloric intake, increased caloric expenditure by the respiratory system and myocardium as well as inability to increase the respiratory work since it is already at maximum capacity due to pulmonary edema.
Option B is incorrect since sucking during feeding in infants is significant exercise effort.
Option C is incorrect. Shortness of breath does occur in congestive heart failure, though this id due to pulmonary edema which decreases the gaseous exchange as the fluid in the pulmonary tissue accumulates. Pulmonary edema also makes the lungs less distensible, requiring the use of intercostals muscles to assist in breathing. Respiratory distress is a cause for easy fatigability as it is an effort to perform, but it is not a manifestation of it.
Option D is incorrect. Cyanosis occurs due to obligatory right to left shunting within th heart, such as with tricuspid atresia. This is not a manifestation of easy fatigability, rather it reflects the presence of a communication between the right heart and the left heart and the inability of deoxygenated blood in the right heart to proceed to the lungs to get oxygenated, and instead being diverted to the left heart to mix with well oxygenated blood, thus causing cyanosis.
Question 15 of 39
15. Question
1 points
Category: History in children with heart disease
A 13 year old girl lost consciousness at school. The story related through her teacher is that the student were watching a game in the field, many of the students, including this patient were standing for at least one hour at noon. The temperature that day was 95 degrees Fahrenheit. Just prior to fainting the young lady was noted to be pale. After fainting, the teacher noted seizure like activity of upper and lower extremities; however, there was no loss of bowel or bladder control. There is no past history of similar episodes.
True statement about this patient is:
Correct
That is Correct!
This appears to be cardioneurogenic syncope which is precipitated by reduction in cardiac pre-load due to dehydration and prolonged standing. The ventricles sense the reduced pre-load and as a compensatory mechanism the myocardium forcefully contracts. This forceful contraction in such individuals falsely stimulates the “C fibers” which are intended to be stimulated in hypertension. Therefore, the brain misinterprets the situation as that of high blood pressure and proceeds to slow the heart rate through the vagus nerve in a misguided effort to lower the blood pressure. Since the blood pressure is already low from reduced pre-load, the further lowering of cardiac output precipitated by bradycardia causes syncope. Once the patient faints, the supine position helps to correct the problem. The only harm may result from head or body injury due to fainting. The transient hypoxia from poor cardiac output may also cause seizure like activity. This is in no way indicative of underlying neurological disorder.
Option A is incorrect as explained above.
Option C is incorrect since seizure like activity is known to occur in cardioneurogenic syncope and EEG is not warranted if no other symptoms or signs are present to indicate neurological disorders.
Option D is incorrect since treatment of cardioneurogenic syncope after a first time occurrence is to avoid dehydration and prolonged standing. Patients are advised to keep well hydrated and increase salt intake if they think that they may encounter excessive perspiration. If these measures fail, then treatment with Florenef or beta blockers may be indicated.
Incorrect
Correct answer is B:
This appears to be cardioneurogenic syncope which is precipitated by reduction in cardiac pre-load due to dehydration and prolonged standing. The ventricles sense the reduced pre-load and as a compensatory mechanism the myocardium forcefully contracts. This forceful contraction in such individuals falsely stimulates the “C fibers” which are intended to be stimulated in hypertension. Therefore, the brain misinterprets the situation as that of high blood pressure and proceeds to slow the heart rate through the vagus nerve in a misguided effort to lower the blood pressure. Since the blood pressure is already low from reduced pre-load, the further lowering of cardiac output precipitated by bradycardia causes syncope. Once the patient faints, the supine position helps to correct the problem. The only harm may result from head or body injury due to fainting. The transient hypoxia from poor cardiac output may also cause seizure like activity. This is in no way indicative of underlying neurological disorder.
Option A is incorrect as explained above.
Option C is incorrect since seizure like activity is known to occur in cardioneurogenic syncope and EEG is not warranted if no other symptoms or signs are present to indicate neurological disorders.
Option D is incorrect since treatment of cardioneurogenic syncope after a first time occurrence is to avoid dehydration and prolonged standing. Patients are advised to keep well hydrated and increase salt intake if they think that they may encounter excessive perspiration. If these measures fail, then treatment with Florenef or beta blockers may be indicated.
Question 16 of 39
16. Question
1 points
Category: History in children with heart disease
A 2 year old is known to have branch pulmonary artery stenosis. The pulmonary arteries are described as small with multiple levels of stenosis, extending to the very distal pulmonary arteries. The cardiac anatomy is otherwise within normal limits. Which one of the following fetal conditions may precipitate this anomaly?
Correct
That is Correct!
Congenital rubella due to maternal infection during gestation may casue peripheral pulmonary stenosis. Peripheral pulmonary stenosis, when mild and transient, is seen in many normal neonates. This is due to small pulmonary arteries secondary to limited pulmonary blood flow in utero, followed by significant increase in blood volume flow upon delivery (8 fold increase).
Option A is incorrect since fetal alcohol syndrome may cause atrial and ventricular septal defects, tetralogy of Fallot and coarctation of the aorta.
Option B is incorrect, since lithium is known to cause Ebstein’s malformation of the tricuspid valve.
Option C is incorrect since maternal diabetes may cause hypertrophic cardiomyopathy, ventricular septal defect, transposition of the great arteries and coarctation of the aorta.
Incorrect
Correct answer is D:
Congenital rubella due to maternal infection during gestation may casue peripheral pulmonary stenosis. Peripheral pulmonary stenosis, when mild and transient, is seen in many normal neonates. This is due to small pulmonary arteries secondary to limited pulmonary blood flow in utero, followed by significant increase in blood volume flow upon delivery (8 fold increase).
Option A is incorrect since fetal alcohol syndrome may cause atrial and ventricular septal defects, tetralogy of Fallot and coarctation of the aorta.
Option B is incorrect, since lithium is known to cause Ebstein’s malformation of the tricuspid valve.
Option C is incorrect since maternal diabetes may cause hypertrophic cardiomyopathy, ventricular septal defect, transposition of the great arteries and coarctation of the aorta.
Question 17 of 39
17. Question
1 points
Category: Cardiovascular physiology, anatomy and pathology
A 2 year old child with double outlet right ventricle (DORV) and severe pulmonary stenosis is asymptomatic, except for easy fatigability. HR is 100 bpm, regular, RR is 35/min, BP is 100/50 in the right arm and O2 saturation is 80%. Despite the low oxygen saturation, there is no visible cyanosis. This could be explained by which one of the following factors:
Correct
That is Correct!
Cyanosis is caused by deoxygenated hemoglobin. Deoxygenated is blue in color, a sufficient concentration of this blue material is required to cause cyanosis to be visible. A concentration of about 2.5 g/dl of deoxygenated hemoglobin, or more will causes cyanosis (i.e. visible discoloration of mucosa and skin).
If one is to assume that a hemoglobin concentration in a patient is 14 g/dl, and the oxygen saturation is 75% (i.e. 75% of the 14 g/dl is oxygenated and 25% is deoxygenated, or 3.5 g/dl is deoxygenated). This will be enough to cause cyanosis.
On the other hand, if the patient has anemia with low hemoglobin concentration, e.g. 6 g/dl, the amount of deoxygenated hemoglobin in this patient will be 1.5g/dl (6X 0.25 = 1.5 g/dl), which is too small of a concentration to cause cyanosis.
Option A is incorrect because PaCO2 levels do not alter levels of deoxygenated hemoglobin.
Options B & D are incorrect. Although in both scenarios there will be less cyanosis, however, this will be due to better oxygen saturation, which is not the case here.
Incorrect
Correct answer is C:
Cyanosis is caused by deoxygenated hemoglobin. Deoxygenated is blue in color, a sufficient concentration of this blue material is required to cause cyanosis to be visible. A concentration of about 2.5 g/dl of deoxygenated hemoglobin, or more will causes cyanosis (i.e. visible discoloration of mucosa and skin).
If one is to assume that a hemoglobin concentration in a patient is 14 g/dl, and the oxygen saturation is 75% (i.e. 75% of the 14 g/dl is oxygenated and 25% is deoxygenated, or 3.5 g/dl is deoxygenated). This will be enough to cause cyanosis.
On the other hand, if the patient has anemia with low hemoglobin concentration, e.g. 6 g/dl, the amount of deoxygenated hemoglobin in this patient will be 1.5g/dl (6X 0.25 = 1.5 g/dl), which is too small of a concentration to cause cyanosis.
Option A is incorrect because PaCO2 levels do not alter levels of deoxygenated hemoglobin.
Options B & D are incorrect. Although in both scenarios there will be less cyanosis, however, this will be due to better oxygen saturation, which is not the case here.
Question 18 of 39
18. Question
1 points
Category: History in children with heart disease
Investigative studies of a three year old child with mental retardation and seizure disorder reveals calcified cranial lesions which increase in intensity with contrast. Examination of the heart reveals a 3/6 systolic ejection murmur at the left mid to left upper sternal border with evidence of right ventricular hypertrophy by electrocardiogram.
Echocardiography will most probably reveal:
Correct
That is Correct!
The child’s presentation and brain imaging is highly suggestive of tuberous sclerosis, an autosomal dominant disease with high spontaneous mutation rate. Brain sclerotic lesion (tubera), skin lesions (depigmented spots) and cardiac tumors (rhabdomyomas) are known to occur. Cardiac tumors are the largest at birth, but thereafter may shrink. Cardiac rhabdomyomas typically affect the ventricular walls and septum.
Option A is incorrect since tuberous sclerosis does not affect the valve tissue.
Option B is incorrect since pulmonary arteries are not affected in this lesion.
Option C is incorrect, again, since cardiac valve tissue is not involved in this lesion. In addition aortic stenosis murmur should be hear best over the right upper sternal border.
Incorrect
Correct answer is D:
The child’s presentation and brain imaging is highly suggestive of tuberous sclerosis, an autosomal dominant disease with high spontaneous mutation rate. Brain sclerotic lesion (tubera), skin lesions (depigmented spots) and cardiac tumors (rhabdomyomas) are known to occur. Cardiac tumors are the largest at birth, but thereafter may shrink. Cardiac rhabdomyomas typically affect the ventricular walls and septum.
Option A is incorrect since tuberous sclerosis does not affect the valve tissue.
Option B is incorrect since pulmonary arteries are not affected in this lesion.
Option C is incorrect, again, since cardiac valve tissue is not involved in this lesion. In addition aortic stenosis murmur should be hear best over the right upper sternal border.
Question 19 of 39
19. Question
1 points
Category: History in children with heart disease
A 14 year old young man presents with 3 episodes of syncope during the past 2 months. Which of the following facts if present in the history of present illness would suggest that the syncopal episode is most probably of cardioneurogenic mechanism?
Correct
That is Correct!
Cardioneurogenic syncope is due to decrease in pre-load, usually associated with dehydration (early in the morning prior to breakfast) or
Incorrect
Correct answer is C:
Cardioneurogenic syncope is due to decrease in pre-load, usually associated with dehydration (early in the morning prior to breakfast) or
Question 20 of 39
20. Question
1 points
Category: History in children with heart disease
A 2 year old girl is failing to thrive. She is otherwise asymptomatic. The child is not taking any medications. Congenital deformity of the hands is noted, there is absent thumb, the father has similar hand anomaly. On examination, there is a 2/6 systolic murmur at the left upper sternal border. First heart sound is normal, second heart sounds splits, without change throughout respiration.
Correct statement about this child is:
Correct
That is Correct!
Holt-Oram is an autosomal dominant disease which includes skeletal abnormalities of the radial side of the forearm and hand, the thumb may be absent. The murmur in this child is consistent with an atrial septal defect which is a known association in Holt-Oram syndrome. These patients are also prone to have ventricular septal defect.
Option A is incorrect since pulmonary stenosis is not a common abnormality in this syndrome and the fixed splitting of the second heart sound indicates atrial septal defect.
Option C is incorrect since the auscultatory findings are inconsistent with ventricular septal defect.
Option D is incorrect since the murmur is not innocent in nature. Innocent heart murmurs are not associated with fixed splitting of the second heart sound.
Incorrect
Correct answer is B:
Holt-Oram is an autosomal dominant disease which includes skeletal abnormalities of the radial side of the forearm and hand, the thumb may be absent. The murmur in this child is consistent with an atrial septal defect which is a known association in Holt-Oram syndrome. These patients are also prone to have ventricular septal defect.
Option A is incorrect since pulmonary stenosis is not a common abnormality in this syndrome and the fixed splitting of the second heart sound indicates atrial septal defect.
Option C is incorrect since the auscultatory findings are inconsistent with ventricular septal defect.
Option D is incorrect since the murmur is not innocent in nature. Innocent heart murmurs are not associated with fixed splitting of the second heart sound.
Question 21 of 39
21. Question
1 points
Category: Physical examination in children with heart disease
A 2 year old with large ventricular septal defect presents with cough and shortness of breath. His current medications are digoxin 5 micrograms/kg /dose PO BID, furosemide 2 mg/kg/dose PO BID and captopril 0.2 mg/kg/dose PO TID. Heart rate is 150 bpm, respiratory rate 45/min, oxygen saturation 95%. On examination the capillary refill is 3 seconds, peripheral pulses are fair. Liver edge is palpated at 5 cm below right costal margin. There is increase in LV and RV impulses and a palpable thrill. In addition to 4/6 holosystolic murmur, there is a 2/4 mid-diastolic murmur.
The capillary refill is prolonged due to:
Correct
That is Correct!
Capillary refill in peripheral tissue, such as fingers and toes, accurately assesses cardiac output. When cardiac output is reduced, catecholamines secreted causes vasoconstriction to non-vital organs such as the gastrointestinal system and peripheral tissue, while preserving flow to vital organs such as the brain, heart and kidneys. The vasoconstriction in peripheral tissue will reflect as pallor and prolonged capillary refill.
Option A is incorrect since venous congestion caused by heart failure will manifest as generalized edema and hepatomegaly, not as vasoconstriction.
Option B is incorrect since the vasodilatation caused by captopril may actually cause brisk capillary refill not reduced capillary refill.
Option C is incorrect since this patient is fully saturated (95%), which suggests that there is no right to left shunting, furthermore, right to left shunting will cause cyanosis with no impact on capillary refill.
Incorrect
Correct answer is D:
Capillary refill in peripheral tissue, such as fingers and toes, accurately assesses cardiac output. When cardiac output is reduced, catecholamines secreted causes vasoconstriction to non-vital organs such as the gastrointestinal system and peripheral tissue, while preserving flow to vital organs such as the brain, heart and kidneys. The vasoconstriction in peripheral tissue will reflect as pallor and prolonged capillary refill.
Option A is incorrect since venous congestion caused by heart failure will manifest as generalized edema and hepatomegaly, not as vasoconstriction.
Option B is incorrect since the vasodilatation caused by captopril may actually cause brisk capillary refill not reduced capillary refill.
Option C is incorrect since this patient is fully saturated (95%), which suggests that there is no right to left shunting, furthermore, right to left shunting will cause cyanosis with no impact on capillary refill.
Question 22 of 39
22. Question
1 points
Category: Physical examination in children with heart disease
A one day old, full term newborn with history of meconium aspiration is in severe respiratory distress requiring significant ventilatory support. Physical examination shows bluish discoloration of the abdomen and lower extremities. Oxygen saturation by pulse oximetry in the right hand is 85%, while that in the lower extremities is 60%. Auscultation reveals normal first heart sound, loud pulmonary component of second heart sound with no significant murmurs. Capillary refill is brisk. In addition to right to left shunting at the ductus arteriosus causing cyanosis of the lower body, this newborn also has:
Correct
That is Correct!
The oxygen desaturation in the lower extremity is expected to be due to right to left shunting at the ductus arteriosus, however, the oxygen desaturation in the upper extremities (85%), which may not produce visible cyanosis, must be caused by right to left shunting at the atrial level or intrapulmonary shunting due to parenchymal lung disease. This patient has no supportive evidence of a ventricular septal defect, which if present will most probably shunt right to left, not left to right. Sever tricuspid regurgitation is indeed present in newborns with pulmonary hypertension; however, this would have produced mitral regurgitation, which is not present in this case. Myocardial dysfunction is unlikely in view of brisk capillary refill.
Incorrect
Correct answer is D:
The oxygen desaturation in the lower extremity is expected to be due to right to left shunting at the ductus arteriosus, however, the oxygen desaturation in the upper extremities (85%), which may not produce visible cyanosis, must be caused by right to left shunting at the atrial level or intrapulmonary shunting due to parenchymal lung disease. This patient has no supportive evidence of a ventricular septal defect, which if present will most probably shunt right to left, not left to right. Sever tricuspid regurgitation is indeed present in newborns with pulmonary hypertension; however, this would have produced mitral regurgitation, which is not present in this case. Myocardial dysfunction is unlikely in view of brisk capillary refill.
Question 23 of 39
23. Question
1 points
Category: Physical examination in children with heart disease
A 12 year old develops syncope for the first time during exercise at school. He was described by observers as being pale. No seizure activity noted. No prior history of syncope. Past medical history and family history are non-contributory. Youngster denies use of medications or illicit drugs. On examination HR is 75 bpm, RR is 20/min, BP in right arm is 100/50 and in leg is 105/45 mmHg. Oxygen saturation is 100%. Brisk capillary refill, no hepatomegaly, the apical impulse is felt at the 7th intercostals space at the anterior axillary line; this correlates with a visible impulse at same site. There is palpable thrill over the upper chest and suprasternal notch. A 4/6 harsh ejection systolic murmur is heard best at the right upper sternal border.
The findings here suggest:
Correct
That is Correct!
The apical impulse in this patient is significantly deviated leftwards and is visible to the naked eye, suggesting left ventricular hypertrophy.
Options B & C are incorrect since right ventricular hypertrophy is manifested as increase impulse at the left lower sternal border.
Option D is incorrect since right atrial enlargement cannot be diagnosed through physical examination, though it could be inferred when there is hepatomegaly secondary to congestive heart failure.
This patient seems to have aortic stenosis.
Incorrect
Correct answer is A:
The apical impulse in this patient is significantly deviated leftwards and is visible to the naked eye, suggesting left ventricular hypertrophy.
Options B & C are incorrect since right ventricular hypertrophy is manifested as increase impulse at the left lower sternal border.
Option D is incorrect since right atrial enlargement cannot be diagnosed through physical examination, though it could be inferred when there is hepatomegaly secondary to congestive heart failure.
This patient seems to have aortic stenosis.
Question 24 of 39
24. Question
1 points
Category: Physical examination in children with heart disease
A 10 year old girl, known to have ventricular septal defect is seen by you because of concern of hypertension. Her parents recently purchased a Doppler based blood pressure measuring device to monitor the father’s essential hypertension. Measurement of the child’s blood pressure using the new device was 125/30 mmHg. Parents are concerned that the child is developing hypertension as well. Your records indicate last year’s blood pressure measurements was 100/65 mmHg.
Correct statement about this child’s blood pressure is:
Correct
That is Correct!
Perimembrenous ventricular septal defects may cause the aortic valve cusps to be involved in the defect resulting in aortic valve deformity and aortic regurgitation. Aortic regurgitation causes drop in diastolic blood pressure due to run off of blood, back into the left ventricle, thus causing a drop in diastolic blood pressure. The regurgitated blood into the left ventricle will contribute to a larger volume being ejected during systole, thus resulting in systolic hypertension. Doppler based devices do cause increase in systolic (not diastolic blood pressure), this patient has high systolic blood pressure, but lower diastolic blood pressure which cannot be explained by the method of measurement. Patients with ventricular septal defect develop increase output to the pulmonary circulation, but decreased output to the systemic circulation (so called increase Qp:Qs ratio). This child’s blood pressure is not normal; the systolic pressure is above the 95th percentile of rage (120 mmHg). The diastolic pressure is too low.
Incorrect
Correct answer is C:
Perimembrenous ventricular septal defects may cause the aortic valve cusps to be involved in the defect resulting in aortic valve deformity and aortic regurgitation. Aortic regurgitation causes drop in diastolic blood pressure due to run off of blood, back into the left ventricle, thus causing a drop in diastolic blood pressure. The regurgitated blood into the left ventricle will contribute to a larger volume being ejected during systole, thus resulting in systolic hypertension. Doppler based devices do cause increase in systolic (not diastolic blood pressure), this patient has high systolic blood pressure, but lower diastolic blood pressure which cannot be explained by the method of measurement. Patients with ventricular septal defect develop increase output to the pulmonary circulation, but decreased output to the systemic circulation (so called increase Qp:Qs ratio). This child’s blood pressure is not normal; the systolic pressure is above the 95th percentile of rage (120 mmHg). The diastolic pressure is too low.
Question 25 of 39
25. Question
1 points
Category: Physical examination in children with heart disease
2-3/6 systolic murmur in a 6 year old is pathological in nature if one of the followings is present:
Correct
That is Correct!
Holosystolic murmurs are pathological since they reflect VSD, TR or MR. Though many people have tricuspid regurgitation by echocardiography, these are not audible as the pressure difference between the right ventricle and atrium are not great, therefore, the Regurgitant jet is not excessively turbulent, and as such is soft and mostly inaudible.
Murmurs which are soft, vibratory in quality and disappear with Valsalva maneuver are typically innocent in nature.
Incorrect
Answer: C
Holosystolic murmurs are pathological since they reflect VSD, TR or MR. Though many people have tricuspid regurgitation by echocardiography, these are not audible as the pressure difference between the right ventricle and atrium are not great, therefore, the Regurgitant jet is not excessively turbulent, and as such is soft and mostly inaudible.
Murmurs which are soft, vibratory in quality and disappear with Valsalva maneuver are typically innocent in nature.
Question 26 of 39
26. Question
1 points
Category: Cardiovascular physiology, anatomy and pathology
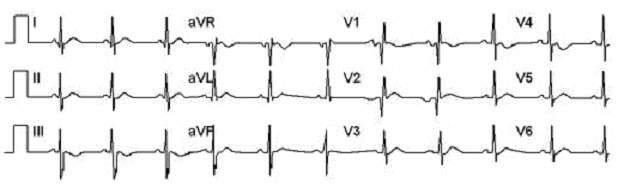
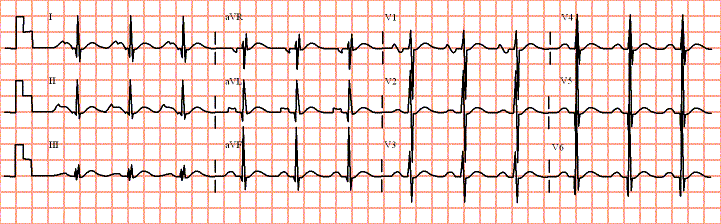
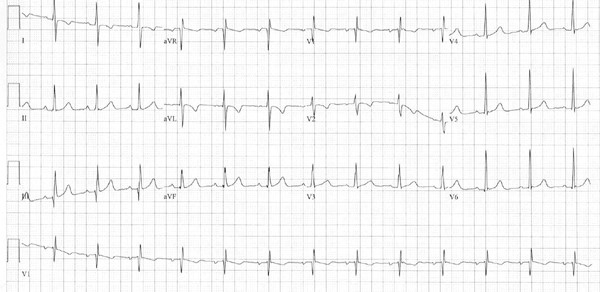
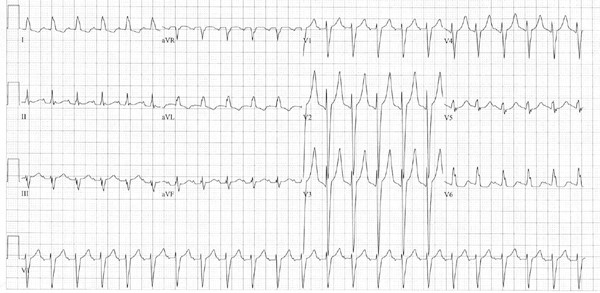
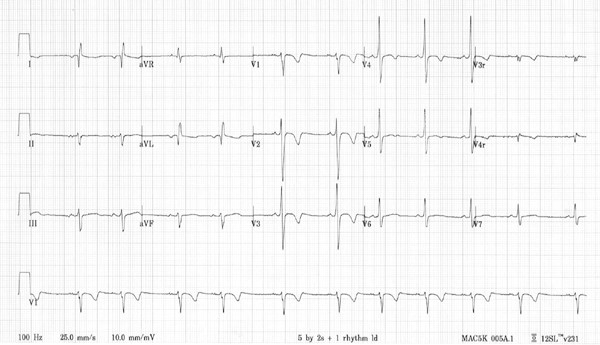
A 2year old boy with a large ASD and hypertrophied muscle bundles in the right ventricular outflow tract with minimal obstruction. Physical examination was remarkable for a 3/6 systolic flow murmur in the left upper sternal border and a 2/4 mid-diastolic murmur in the left lower sternal border. S2 was split without variation throughout the respiratory cycle. Surgical closure of the ASD and resection of hypertrophied muscle bundles was preformed. Physical examination post-operatively indicates no residual murmur; however, S2 continues to have fixed splitting though-out the respiratory cycle. ECG is shown below (click to enlarge image):
E2
E2
What is causing the fixed splitting of S2 post-operatively?
Correct
That is Correct!
Fixed splitting of second heart sound in patients with ASD is caused by the constant delay in closure of the pulmonary valve due to excessive blood flow through it as a result of the ASD. Once the ASD is closed, murmurs and fixed splitting of the second heart sound should be resolved. Another cause for fixed splitting of the second heart sound is delayed start of RV contractility in systole, such as with right bundle branch block, this will cause delay in pulmonary closure throughout the respiratory cycle.
This patient underwent closure of ASD as well as resection of hypertrophied muscle bundles. The former caused the resolution of murmurs, however, the latter could cause right bundle branch block which is seen in the ECG. This will also cause delayed closure of the pulmonary valve, due to a different mechanism, resulting in continuation of fixed splitting of the second heart sound.
Incorrect
Correct answer is C:
Fixed splitting of second heart sound in patients with ASD is caused by the constant delay in closure of the pulmonary valve due to excessive blood flow through it as a result of the ASD. Once the ASD is closed, murmurs and fixed splitting of the second heart sound should be resolved. Another cause for fixed splitting of the second heart sound is delayed start of RV contractility in systole, such as with right bundle branch block, this will cause delay in pulmonary closure throughout the respiratory cycle.
This patient underwent closure of ASD as well as resection of hypertrophied muscle bundles. The former caused the resolution of murmurs, however, the latter could cause right bundle branch block which is seen in the ECG. This will also cause delayed closure of the pulmonary valve, due to a different mechanism, resulting in continuation of fixed splitting of the second heart sound.
Question 27 of 39
27. Question
1 points
Category: Cardiovascular physiology, anatomy and pathology
Increase in pulse pressure further away from the heart
A 4 year old who is seen in the emergency room for a laceration of the skin over the chin secondary to a fall. The child is active with no history of easy fatigability, shortness of breath or cyanosis. Physical examination demonstrates HR of 100 bpm, regular rhythm. RR is 25/min. BP in right arm is 100/60 and in left leg 110/50. Peripheral pulses are easy to palpate, dorsalis pedis pulses appear to be easier to palpate that brachial pulses in the right upper arm. A 2/6 vibratory systolic murmur at left upper sternal brooder with no appreciable radiation is heard. This murmur disappears in upright position and with Valsalva maneuver.
Correct statement regarding the pulses in upper and lower extremity is:
Correct
That is Correct!
Pulse accentuation is a phenomenon of systemic blood vessels. Due to recoil of vessels, the systolic blood pressure increases further away from the heart. In addition the diastolic blood pressure decreases in the more distal circulation. This increase in systolic pressure and decrease in diastolic pressure in more distal blood vessels when compared to blood vessels more proximal to the heart creates a wider pulse pressure, which enables easier palpation.
Option A is incorrect since systolic BP decreases and not increases in lower extremities versus upper extremities in patients with coarctation of the aorta.
Option C is incorrect since systolic BP increases in more distal circulation.
Option D is incorrect since mean systemic BP continues to decrease further away from the heart which is what enables blood to move foreword. In a circulation, proximal mean pressures have to always be more than distal pressures.
Incorrect
Correct statement is B
Pulse accentuation is a phenomenon of systemic blood vessels. Due to recoil of vessels, the systolic blood pressure increases further away from the heart. In addition the diastolic blood pressure decreases in the more distal circulation. This increase in systolic pressure and decrease in diastolic pressure in more distal blood vessels when compared to blood vessels more proximal to the heart creates a wider pulse pressure, which enables easier palpation.
Option A is incorrect since systolic BP decreases and not increases in lower extremities versus upper extremities in patients with coarctation of the aorta.
Option C is incorrect since systolic BP increases in more distal circulation.
Option D is incorrect since mean systemic BP continues to decrease further away from the heart which is what enables blood to move foreword. In a circulation, proximal mean pressures have to always be more than distal pressures.
Question 28 of 39
28. Question
1 points
Category: History in children with heart disease
A 12 year old with un-repaired tetralogy of Fallot is cyanotic with clubbing of the digits. He tends to squat when fatigued. Past medical history is significant for a cerebral abscess few years ago with mild residual weakness of the right arm and leg. HR is 75 bpm, regular. RR is 20/min. BP in right arm is 110/40 mmHg. Oxygen saturation is 70%. On auscultation, second heart is single with a 4/6 harsh systolic murmur heard best over the left upper sternal border.
The cause of squatting in this patient is:
Correct
That is Correct!
Children with tetralogy of Fallot learn to squat when fatigued to increase their systemic blood’s oxygen saturation. This is thought to be caused by the kinking of femoral arteries in the groin by squatting. This will increase the systemic vascular resistance, thus forcing more blood across the narrow right ventricular outflow tract and stenotic pulmonary valve. An additional benefit may be due to the effect of squatting n increase pre-load of the right ventricle due to the increased intra-abdominal pressure. This increase pre-load will tend to stretch the right ventricle, thus allowing more blood to flow as=cross the right ventricular outflow tract and pulmonary valve into the lungs, thus improving oxygen saturation.
Option A is incorrect since this episodic phenomenon does not appear to be of neurological origin.
Option B is incorrect since in tetralogy of Fallot there is less pulmonary blood flow due to severe pulmonary valvar and right ventricular outflow stenosis. Therefore, pulmonary edema is unlikely.
Option C is incorrect since this does not appear to be consistent with any known orthopedic ailment.
Incorrect
Correct answer is D
Children with tetralogy of Fallot learn to squat when fatigued to increase their systemic blood’s oxygen saturation. This is thought to be caused by the kinking of femoral arteries in the groin by squatting. This will increase the systemic vascular resistance, thus forcing more blood across the narrow right ventricular outflow tract and stenotic pulmonary valve. An additional benefit may be due to the effect of squatting n increase pre-load of the right ventricle due to the increased intra-abdominal pressure. This increase pre-load will tend to stretch the right ventricle, thus allowing more blood to flow accross the right ventricular outflow tract and pulmonary valve into the lungs, thus improving oxygen saturation.
Option A is incorrect since this episodic phenomenon does not appear to be of neurological origin.
Option B is incorrect since in tetralogy of Fallot there is less pulmonary blood flow due to severe pulmonary valvar and right ventricular outflow stenosis. Therefore, pulmonary edema is unlikely.
Option C is incorrect since this does not appear to be consistent with any known orthopedic ailment.
Question 29 of 39
29. Question
1 points
Category: History in children with heart disease
History of deafness in a child with syncope may indicate
A 6 year old presents with syncope while watching TV. The child is known to be deaf, but otherwise healthy. Family history is significant for an uncle with deafness who died suddenly at 16 years of age.
An important initial step in assessing this child is:
Correct
That is Correct!
This child has Jervell and Lange-Neilsen syndrome. This is an autosomal recessive disease with nerve deafness and prolonged QT interval, which may cause ventricular tachycardia (Torsades de pointes). The syncope in this child is most probably related to an event of tachyarrhythmia. ECG will show prolonged QTc.
Option A is incorrect since an MRI will not be productive.
Option B is incorrect since the heart will appear normal in between tachyarrhythmia events.
Option C is incorrect since the syncope occurred while the child is sitting; therefore, it is unlikely to be related to cardioneurogenic syncope.
Incorrect
Correct answer is D:
This child has Jervell and Lange-Neilsen syndrome. This is an autosomal recessive disease with nerve deafness and prolonged QT interval, which may cause ventricular tachycardia (Torsades de pointes). The syncope in this child is most probably related to an event of tachyarrhythmia. ECG will show prolonged QTc.
Option A is incorrect since an MRI will not be productive.
Option B is incorrect since the heart will appear normal in between tachyarrhythmia events.
Option C is incorrect since the syncope occurred while the child is sitting; therefore, it is unlikely to be related to cardioneurogenic syncope.
Question 30 of 39
30. Question
1 points
Category: History in children with heart disease
A 6 year old girl had surgical closure of a secundum atrial septal defect (ASD). What historical information should indicate that the patient does not require subacute bacterial endocarditis (SBE) prophylaxis for potential bacteremic procedures, such as dental cleaning?
Correct
That is Correct!
SBE prophylaxis for ASD is not required for secundum ASD prior to repair and 6 months after repair. SBE prophylaxis is needed for 6 months after closure of ASD (surgical closure or device closure). The use of prosthetic material in closure of an ASD or the use of primary closure versus patch closure do not alter these recommendations, since 6 months of time allows for endothelialization of the closed ASD and consequently elimination of need for prophylaxis.
Incorrect
Correct answer is C:
SBE prophylaxis for ASD is not required for secundum ASD prior to repair and 6 months after repair. SBE prophylaxis is needed for 6 months after closure of ASD (surgical closure or device closure). The use of prosthetic material in closure of an ASD or the use of primary closure versus patch closure do not alter these recommendations, since 6 months of time allows for endothelialization of the closed ASD and consequently elimination of need for prophylaxis.
Question 31 of 39
31. Question
1 points
Category: Physical examination in children with heart disease
In a 13 year old girl with dilated cardiomyopathy, percussion of the chest could help in:
Correct
That is Correct!
Percussion of the chest may be helpful when assessing the lungs, however, its use in cardiac assessment is very limited.
Option A is incorrect since it is not possible to assess the heart size with any accuracy using percussion. Chest x-ray and echocardiography are much more accurate for this purpose.
Option B is incorrect since extent of mitral regurgitation can only be assessed by echocardiography or angiography.
Option D is incorrect since left ventricular hypertrophy may be suggested through palpation of an increased and leftward displaced apical impulse but not by percussion.
Incorrect
Correct answer is C:
Percussion of the chest may be helpful when assessing the lungs, however, its use in cardiac assessment is very limited.
Option A is incorrect since it is not possible to assess the heart size with any accuracy using percussion. Chest x-ray and echocardiography are much more accurate for this purpose.
Option B is incorrect since extent of mitral regurgitation can only be assessed by echocardiography or angiography.
Option D is incorrect since left ventricular hypertrophy may be suggested through palpation of an increased and leftward displaced apical impulse but not by percussion.
Question 32 of 39
32. Question
1 points
Category: Physical examination in children with heart disease
A 14 year old African American female who is a member of the schools basketball team is being evaluated for clearance to participate in the school’s next year basketball team. There are no symptoms relating to the cardiovascular system. Vital signs are within normal limits. Physical examination shows a healthy appearing young lady, Tanner stage 4. A 2/6 systolic murmur is heard over the left and right sides of the chest. S1 and S2 are within normal limits. No appreciable change in the quality of the murmur with valsalva or upright position. ECG and CXR are normal.
Correct statement regarding this case is:
Correct
That is Correct!
Developing breasts in teen age girls may produce systolic flow murmurs relating to increased circulation, called mammary soufflé. This is particularly noted in lactating women as the rapid breast tissue growth induces increased blood flow, resulting in a murmur.
Innocent heart murmurs, as in this case are heard throughout childhood and young adulthood, though more common in younger children. Systemic to pulmonary collaterals are unlikely in an otherwise healthy person with no other signs or symptoms of heart disease. Collaterals are noted in some patients with pulmonary atresia. Peripheral pulmonary stenosis is normal in neonatal period and early infancy. Peripheral pulmonary stenosis beyond 3 months of age is always pathological, as seen inpatients with William’s syndrome, congenital Rubella and Noonan’s syndrome.
Incorrect
Answer: B
Developing breasts in teen age girls may produce systolic flow murmurs relating to increased circulation, called mammary soufflé. This is particularly noted in lactating women as the rapid breast tissue growth induces increased blood flow, resulting in a murmur.
Innocent heart murmurs, as in this case are heard throughout childhood and young adulthood, though more common in younger children. Systemic to pulmonary collaterals are unlikely in an otherwise healthy person with no other signs or symptoms of heart disease. Collaterals are noted in some patients with pulmonary atresia. Peripheral pulmonary stenosis is normal in neonatal period and early infancy. Peripheral pulmonary stenosis beyond 3 months of age is always pathological, as seen inpatients with William’s syndrome, congenital Rubella and Noonan’s syndrome.
Question 33 of 39
33. Question
4 points
Category: Physical examination in children with heart disease
When interrogating a heart murmur in a 4 year old, valsalva maneuver is performed by:
Correct
That is Correct!
Valsalva maneuver is achieved when the intrathoracic pressure is increased. A child of this age may cooperate if he is pretending to blow up a balloon by placing his thumb in his mouth and blow without actually letting any air out. In babies, the method described in “B” can be attempted. Asking a child of this age to pretend having a bowel movement is not always possible. They may not comprehend the request, or worse, comply and do have a bowel movement!
Incorrect
Answer: C
Valsalva maneuver is achieved when the intrathoracic pressure is increased. A child of this age may cooperate if he is pretending to blow up a balloon by placing his thumb in his mouth and blow without actually letting any air out. In babies, the method described in “B” can be attempted. Asking a child of this age to pretend having a bowel movement is not always possible. They may not comprehend the request, or worse, comply and do have a bowel movement!
Question 34 of 39
34. Question
1 points
Category: Physical examination in children with heart disease
The murmur of coarctation of the aorta, heard over the back, appears to extend into diastole, this is because:
Correct
That is Correct!
Systole and diastole is determined in auscultation through using the first and second heart sounds as reference points. The stroke volume ejected by the left ventricle in systole will require few milliseconds prior to reaching the stenotic area of the aortic arch in coarctation of the aorta, this will result in a murmur generated, appearing as if it is in systole and early diastole.
Although coarctation of the aorta is occasionally associated with collaterals, which produce continuous murmur, this is NOT a frequent occurrence. Mitral stenosis may be associated with coarctation. However, the diastolic murmur caused by mitral stenosis is heard at the cardiac apex and not over the back. Similarly, aortic regurgitation is heard over the precordium, usually in the mid-sternum, not over the back.
Incorrect
Answer: C
Systole and diastole is determined in auscultation through using the first and second heart sounds as reference points. The stroke volume ejected by the left ventricle in systole will require few milliseconds prior to reaching the stenotic area of the aortic arch in coarctation of the aorta, this will result in a murmur generated, appearing as if it is in systole and early diastole.
Although coarctation of the aorta is occasionally associated with collaterals, which produce continuous murmur, this is NOT a frequent occurrence. Mitral stenosis may be associated with coarctation. However, the diastolic murmur caused by mitral stenosis is heard at the cardiac apex and not over the back. Similarly, aortic regurgitation is heard over the precordium, usually in the mid-sternum, not over the back.
Question 35 of 39
35. Question
1 points
Category: Physical examination in children with heart disease
A one month old infant with severe congestive heart failure has cardiomegaly by chest x-ray. Echocardiography shows normal cardiac anatomy with severe dilation of all cardiac chambers. A complete examination of this child may reveal which one of the following?
Correct
That is Correct!
Left to right shunting at peripheral vasculature, such as hepatic or cranial arterio-venous malformation, will result in volume overload of the heart.. This will manifest as cardiomegaly and congestive heart failure. Therefore, when suspecting high cardiac output failure, thorough examination should include auscultation of the head and abdomen.
Incorrect
Correct answer is B:
Left to right shunting at peripheral vasculature, such as hepatic or cranial arterio-venous malformation, will result in volume overload of the heart. This will manifest as cardiomegaly and congestive heart failure. Therefore, when suspecting high cardiac output failure, thorough examination should include auscultation of the head and abdomen.
Question 36 of 39
36. Question
1 points
Category: Physical examination in children with heart disease
While performing cardiac auscultation, the second heart sound could be heard to split into two components during inspiration. The first component of the second heart sound is the aortic valve closure, while the second component is the pulmonary valve closure. What causes the pulmonary valve to close second to the aortic valve?
Correct
That is Correct!
The left His bundle branch is shorter than the right, therefore, the left ventricle is stimulated few milliseconds before the right, resulting in completion of systole in the left ventricle prior to that of the right ventricle. Consequently the aortic valve closes first.
Incorrect
Correct answer is D:
The left His bundle branch is shorter than the right, therefore, the left ventricle is stimulated few milliseconds before the right, resulting in completion of systole in the left ventricle prior to that of the right ventricle. Consequently the aortic valve closes first.
Question 37 of 39
37. Question
1 points
Category: Physical examination in children with heart disease
During inspiration, the second heart sound is found to be split, while during expiration the second heart sound is single in a six year old undergoing physical examination. This finding is caused by which one of the following?
Correct
That is Correct!
The negative intrathoracic pressure caused by inspiration results in an increase in blood return to the right heart. This will cause the pulmonary valve to stay open even later than usual, resulting in splitting of the second heart sound. During expiration, less blood is returned to the right heart and more blood return from the lung to the left heart, causing the pulmonary valve to close early and the aortic valve to close late, thus occurring at the same time and resulting in a single second heart sound. Atrial septal defect will cause the pulmonary valve to always close later than the aortic valve, regardless of the respiratory cycle (fixed splitting). Early depolarization of the left ventricle is a constant phenomenon throughout the respiratory cycle. It is this phenomenon that causes the aortic valve to close earlier than the pulmonary valve. Aortic valve stenosis, if severe, will cause delayed closure of the aortic valve. This will cause paradoxical splitting of the second heart sound, i.e. single heart sound in inspiration and reverse splitting in expiration.
Incorrect
Correct answer is A:
The negative intrathoracic pressure caused by inspiration results in an increase in blood return to the right heart. This will cause the pulmonary valve to stay open even later than usual, resulting in splitting of the second heart sound. During expiration, less blood is returned to the right heart and more blood return from the lung to the left heart, causing the pulmonary valve to close early and the aortic valve to close late, thus occurring at the same time and resulting in a single second heart sound. Atrial septal defect will cause the pulmonary valve to always close later than the aortic valve, regardless of the respiratory cycle (fixed splitting). Early depolarization of the left ventricle is a constant phenomenon throughout the respiratory cycle. It is this phenomenon that causes the aortic valve to close earlier than the pulmonary valve. Aortic valve stenosis, if severe, will cause delayed closure of the aortic valve. This will cause paradoxical splitting of the second heart sound, i.e. single heart sound in inspiration and reverse splitting in expiration.
Question 38 of 39
38. Question
1 points
Category: Physical examination in children with heart disease
A harsh 3/6 ejection systolic murmur, heard loudest at the left sternal border could be caused by all of the following, except:
Correct
That is Correct!
All the listed lesion cause systolic murmurs, the pulmonary and right ventricular outflow tract murmurs are identical. Ventricular septal defect murmurs are typically holosystolic, except when they are small muscular, which may cause the murmur to cease early due to obliteration of orifice of defect by contracting ventricular muscles. The aortic valve stenosis murmur is ejection systolic, but is heard loudest at the right upper sternal border.
Incorrect
Correct answer is A:
All the listed lesion cause systolic murmurs, the pulmonary and right ventricular outflow tract murmurs are identical. Ventricular septal defect murmurs are typically holosystolic, except when they are small muscular, which may cause the murmur to cease early due to obliteration of orifice of defect by contracting ventricular muscles. The aortic valve stenosis murmur is ejection systolic, but is heard loudest at the right upper sternal border.
Question 39 of 39
39. Question
1 points
Category: Physical examination in children with heart disease
A diastolic murmur is heard over the left lower sternal border. Which of the following additional findings would help differentiate tricuspid stenosis from atrial septal defect?
Correct
That is Correct!
Turbulence of blood flow through the tricuspid valve due to narrow orifice such as in tricuspid stenosis, or due to increase volume of blood flow such as in atrial septal defect will cause mid-diastolic murmur at the left lower sternal border (tricuspid area). The quality of the murmur and its timing is identical in both conditions, however, in atrial septal defect, there is additionally a systolic ejection murmur over the left upper sternal border (pulmonic area) and fixed splitting of second heart sound throughout the respiratory cycle.
Incorrect
Correct answer is C:
Turbulence of blood flow through the tricuspid valve due to narrow orifice such as in tricuspid stenosis, or due to increase volume of blood flow such as in atrial septal defect will cause mid-diastolic murmur at the left lower sternal border (tricuspid area). The quality of the murmur and its timing is identical in both conditions, however, in atrial septal defect, there is additionally a systolic ejection murmur over the left upper sternal border (pulmonic area) and fixed splitting of second heart sound throughout the respiratory cycle.
Time limit: 0
Quiz-summary
0 of 45 questions completed
Questions:
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
Information
CCHD Exam – Part II
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You must sign in or sign up to start the quiz.
You have to finish following quiz, to start this quiz:
Results
0 of 45 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 points, (0)
Average score
Your score
Categories
CXR in children with heart disease0%
ECG0%
Heart Murmurs0%
Congratulations on a job well done!
Your result has been entered into leaderboard
Loading
maximum of 45 points
Pos.
Name
Entered on
Points
Result
Table is loading
No data available
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
Answered
Review
Question 1 of 45
1. Question
1 points
Category: Heart Murmurs
A 16 year old girl experienced syncope while getting ready to go to school early in the morning. The syncopal episode was witnessed by her mother, a nurse, who states that the young lady first became pale and nauseous; her heart rate at that time was 40 bpm, regular. After a minute or two, the young lady was awake and feeling well. This episode reoccurred 3 more times during the next 2 months. The child was seen by a physician who, after investigative studies prescribed Atenolol, a beta blocker. The young lady is doing well now with no episodes of syncope recently. Mother, who is known to have essential hypertension, is also treated with same medication.
Which of the following statements is correct regarding the use of beta blockers in this patient?
Correct
That is Correct!
This young lady’s presentation is consistent with Cardioneurogenic syncope. Patient is most vulnerable when dehydrated, such as early in the morning. Syncope may be preceded by sense of nausea or disorientation, followed by fainting. The pathophysiology is shown in the diagram below. Beta blockers are used to prevent the hypercontractility from occurring, thus breaking the cycle even before bradycardia occurs. Severe hypertension may cause reflex bradycardia, but this does not appear to be the case here. Bradycardia associated with hypertension is not associated with syncope.
Incorrect
Correct answer is C:
This young lady’s presentation is consistent with Cardioneurogenic syncope. Patient is most vulnerable when dehydrated, such as early in the morning. Syncope may be preceded by sense of nausea or disorientation, followed by fainting. Beta blockers are used to prevent the hypercontractility from occurring, thus breaking the cycle even before bradycardia occurs. Severe hypertension may cause reflex bradycardia, but this does not appear to be the case here. Bradycardia associated with hypertension is not associated with syncope.
Question 2 of 45
2. Question
1 points
Category: CXR in children with heart disease
CXR
Accurate description of the cardiac silhouette below is:
e7
e7
Correct
That is Correct!
The heart size is within normal limits and the cardiac silhouette is normal.
Incorrect
Correct answer is C:
The heart size is within normal limits and the cardiac silhouette is normal.
Question 3 of 45
3. Question
1 points
Category: CXR in children with heart disease
CXR
The mass in the right upper chest in the chest x-ray below is probably due to which one of the following?
e10
e10
Correct
That is Correct!
This patient has tetralogy of Fallot with pulmonary atresia and collaterals from subclavian arteries to pulmonary circulation resulting in an abnormal shadow, above that of the heart. Pericardial effusion enlarges the heart and pleural effusion surrounds the lung fields, neither of these conditions would cause a mass like effect in the right upper chest.
Incorrect
Correct answer is B:
This patient has tetralogy of Fallot with pulmonary atresia and collaterals from subclavian arteries to pulmonary circulation resulting in an abnormal shadow, above that of the heart. Pericardial effusion enlarges the heart and pleural effusion surrounds the lung fields, neither of these conditions would cause a mass like effect in the right upper chest.
Question 4 of 45
4. Question
1 points
Category: Heart Murmurs
Pathological versus innocent heart murmur
Of the following case scenarios, which case suggests that the murmur is pathological in origin?
Correct
That is Correct!
The child in the case scenario “A” has typical stigmata of Down syndrome. 40% of these children are known to have congenital heart disease, mostly complete atrio-ventricular canal (AVC) defect. However, this child appears to have peripheral pulmonary stenosis, a normal finding in children less than 6 weeks of age. The murmur of AVC defect is that of a VSD, i.e. holosystolic and harsh.
The child in case scenario “B” has the features of Holt-Oram syndrome. This anomaly affects skeletal and cardiovascular systems. Patients have hypoplasia of lateral arm skeletal structures as well cardiac anomalies. The most encountered heart lesion is atrial septal defect, which appears to be the case here. The murmur is secondary to increase pulmonary valve blood flow and the fixed splitting of the second heart sound is due to constant increase in blood flow due to the ASD.
The patient in case scenario “C” is pregnant. Here fetus has congenital heart disease, but there is no clinical evidence that the mother has any cardiac problem. The murmur heard in this patient is a “mammary soufflé” which is heard in women with enlarging breast, as encountered in teenagers and pregnancy.
The child in case scenario “D” most probably has reactive airway disease. The bronchodilators used causes tachycardia and occasionally premature atrial contractions, this may explain the irregularity of the heart rhythm. The murmur described here is consistent with a venous hum since it is supra-clavicular not sub-clavicular which would make one think of PDA. The murmur increases in intensity in upright position because of increase venous return through the jugular veins when standing, this murmur should disappear if pressure is applied to that side of the neck.
Incorrect
Correct answer is B:
The child in the case scenario “A” has typical stigmata of Down syndrome. 40% of these children are known to have congenital heart disease, mostly complete atrio-ventricular canal (AVC) defect. However, this child appears to have peripheral pulmonary stenosis, a normal finding in children less than 6 weeks of age. The murmur of AVC defect is that of a VSD, i.e. holosystolic and harsh.
The child in case scenario “B” has the features of Holt-Oram syndrome. This anomaly affects skeletal and cardiovascular systems. Patients have hypoplasia of lateral arm skeletal structures as well cardiac anomalies. The most encountered heart lesion is atrial septal defect, which appears to be the case here. The murmur is secondary to increase pulmonary valve blood flow and the fixed splitting of the second heart sound is due to constant increase in blood flow due to the ASD.
The patient in case scenario “C” is pregnant. Here fetus has congenital heart disease, but there is no clinical evidence that the mother has any cardiac problem. The murmur heard in this patient is a “mammary soufflé” which is heard in women with enlarging breast, as encountered in teenagers and pregnancy.
The child in case scenario “D” most probably has reactive airway disease. The bronchodilators used causes tachycardia and occasionally premature atrial contractions, this may explain the irregularity of the heart rhythm. The murmur described here is consistent with a venous hum since it is supra-clavicular not sub-clavicular which would make one think of PDA. The murmur increases in intensity in upright position because of increase venous return through the jugular veins when standing, this murmur should disappear if pressure is applied to that side of the neck.
Question 5 of 45
5. Question
1 points
Category: Heart Murmurs
Identify murmur
To hear the murmur referred to in this question, click on the sound clip below.
Clues: 6 months, thriving well, normal heart size and pulmonary blood flow by chest x-ray.
Describe heart sounds/murmur in this patient:
Correct
That is Correct!
Modified in my version to be B (based on the scenario)
Normal heart sounds, no murmur.
Incorrect
Correct answer is A.
Modified in my version to be B (based on the scenario)
Normal heart sounds, no murmur.
Question 6 of 45
6. Question
1 points
Category: Heart Murmurs
Identify murmur
To hear the murmur referred to in this question, click on the sound clip below.
Clues: Shortness of breath, cardiomegaly, skeletal abnormality of thumb in patient and father.
What is the diagnosis?
Correct
That is Correct!
There is a systolic ejection murmur with fixed splitting of second heart sound a soft mid-diastolic murmur. The patient appears to have Holt-Oram syndrome.
Incorrect
Correct answer is B
There is a systolic ejection murmur with fixed splitting of second heart sound a soft mid-diastolic murmur. The patient appears to have Holt-Oram syndrome.
Question 7 of 45
7. Question
1 points
Category: Heart Murmurs
Identify murmur
To hear the murmur referred to in this question, click on the sound clip below.
Clues: prominence of the left heart border, below aortic knob on chest x-ray.
What type of murmur is this?
Correct
That is Correct!
Diagnosis is pulmonary stenosis. Same answer, changed scenario
Incorrect
Correct answer is C
Diagnosis is pulmonary stenosis. Same answer, changed scenario
Question 8 of 45
8. Question
1 points
Category: Heart Murmurs
Identify murmur
To hear the murmur referred to in this question, click on the sound clip below.
Clues: 8 months old with congestive heart failure and increase pulmonary blood flow by chest x-ray.
What type of murmur is this?
Correct
That is Correct!
Diagnosis is patent ductus arteriosus. Same answer, changed scenario
Incorrect
Correct answer is A
Diagnosis is patent ductus arteriosus. Same answer, changed scenario
Question 9 of 45
9. Question
1 points
Category: Heart Murmurs
Identify murmur
To hear the murmur referred to in this question, click on the sound clip below.
Clues: Cardiogenic shock
What is the diagnosis?
Correct
That is Correct!
The murmur is ejection systolic murmur with normal first and second heart sounds. Same answer, changed scenario
Incorrect
Correct answer is A
The murmur is ejection systolic murmur with normal first and second heart sounds. Same answer, changed scenario
Question 10 of 45
10. Question
1 points
Category: Heart Murmurs
Identify murmur
To hear the murmur referred to in this question, click on the sound clip below.
Clues: Giant p waves on ECG
What is the diagnosis?
Correct
That is Correct!
Ebstein’s malformation may have a variety of murmurs, here there is fixed splitting of second heart sound. Same answer, changed scenario
Incorrect
Correct answer is B
Ebstein’s malformation may have a variety of murmurs, here there is fixed splitting of second heart sound. Same answer, changed scenario
Question 11 of 45
11. Question
1 points
Category: Heart Murmurs
Identify murmur
To hear the murmur referred to in this question, click on the sound clip below.
Clues: 13 years old with history of rheumatic heart disease and poor medical follow up.
What does this murmur suggest?
Correct
That is Correct!
The murmur is diastolic; this would be heard loudest at the apical region. Same answer, changed scenario
Incorrect
Correct answer is C
The murmur is diastolic; this would be heard loudest at the apical region. Same answer, changed scenario
Question 12 of 45
12. Question
1 points
Category: Heart Murmurs
Identify murmur
To hear the murmur referred to in this question, click on the sound clip below.
Clues: healthy 12 year old girl with occasional chest pain.
Which cardiac valve is the culprit in this case?
Correct
That is Correct!
The murmur (systolic click followed by a murmur) is of mitral valve prolapse, known to be associated with chest pain. Same answer, changed scenario
Incorrect
Correct answer is A
The murmur (systolic click followed by a murmur) is of mitral valve prolapse, known to be associated with chest pain. Same answer, changed scenario
Question 13 of 45
13. Question
1 points
Category: Heart Murmurs
Identify murmur
To hear the murmur referred to in this question, click on the sound clip below.
Clues: 18 months old, was in congestive heart failure earlier in infancy, now asymptomatic
What is the diagnosis?
Correct
That is Correct!
The murmur is holosystolic. The defect appears to be smaller now, thus lack of symptoms. Same answer, changed scenario
Incorrect
Correct answer is D
The murmur is holosystolic. The defect appears to be smaller now, thus lack of symptoms. Same answer, changed scenario
Question 14 of 45
14. Question
1 points
Category: Heart Murmurs
Identify murmur
To hear the murmur referred to in this question, click on the sound clip below.
Clues: Had ventricular septal defect closed 2 years ago
What type of murmur is this?
Correct
That is Correct!
This patient has aortic regurgitation as complication to ventricular septal defect. I modified the scenario and the choices. Correct answer is still D.
Incorrect
Correct answer is D
This patient has aortic regurgitation as complication to ventricular septal defect. I modified the scenario and the choices. Correct answer is still D.
Question 15 of 45
15. Question
1 points
Category: Heart Murmurs
Identify murmur
To hear the murmur referred to in this question, click on the sound clip below.
Clues: easy fatigability and shortness of breath in a 12 year old with cardiomegaly and increase pulmonary blood flow by chest x-ray.
What do you expect an electrocardiogram to show in a patient with this murmur?
Correct
That is Correct!
The murmur is that of an atrial septal defect. Same answer, changed scenario
Incorrect
Correct answer is B
The murmur is that of an atrial septal defect. Same answer, changed scenario
Question 16 of 45
16. Question
1 points
Category: Heart Murmurs
Identify murmur
To hear the murmur referred to in this question, click on the sound clip below.
Clues: 2 years old with normal physical examination except for the murmur. Chest x-ray and electrocardiogram are normal.
Diagnosis is:
Correct
That is Correct!
The murmur is a soft systolic murmur, suggestive of Still’s (aortic flow innocent murmur). Peripheral pulmonary stenosis is not normal at this age. Same answer, changed scenario
Incorrect
Correct answer is A
The murmur is a soft systolic murmur, suggestive of Still’s (aortic flow innocent murmur). Peripheral pulmonary stenosis is not normal at this age. Same answer, changed scenario
Question 17 of 45
17. Question
1 points
Category: Heart Murmurs
Identify murmur
To hear the murmur referred to in this question, click on the sound clip below:
Clues: s/p surgical repair of complete atrio-ventricular canal defect
What is the murmur caused by?
Correct
That is Correct!
The murmur is holosystolic; this would most probably be loudest at the apex. Same answer, changed scenario
Incorrect
Correct answer is B
The murmur is holosystolic; this would most probably be loudest at the apex. Same answer, changed scenario
Question 18 of 45
18. Question
1 points
Category: CXR in children with heart disease
CXR
The changes in the CXR below are most probably precipitated by which of the following cardiac lesions:
Correct
That is Correct!
The CXR shows biventricular enlargement, increase pulmonary blood flow and haziness of the right lung field, which may suggest right pleural effusion. In aortic stenosis the LV is enlarged, causing the apex to be downwards towards the diaphragm as well as leftward displacement. Pulmonary stenosis causes right ventricular hypertrophy causing the left ventricular apex to be uplifted, which is noted here, however, the cardiac silhouette is typically not enlarged in the antero-posterior projection. Pulmonary vascular markings are normal in both aortic and pulmonary stenosis. Atrial septal defect does not cause left ventricular enlargement.
Incorrect
xxCorrect answer is A:
The CXR shows biventricular enlargement, increase pulmonary blood flow and haziness of the right lung field, which may suggest right pleural effusion. In aortic stenosis the LV is enlarged, causing the apex to be downwards towards the diaphragm as well as leftward displacement. Pulmonary stenosis causes right ventricular hypertrophy causing the left ventricular apex to be uplifted, which is noted here, however, the cardiac silhouette is typically not enlarged in the antero-posterior projection. Pulmonary vascular markings are normal in both aortic and pulmonary stenosis. Atrial septal defect does not cause left ventricular enlargement.
Question 19 of 45
19. Question
1 points
Category: CXR in children with heart disease
CXR
The changes in the CXR below are most probably precipitated by which of the following cardiac lesions:
E2
E2
Correct
That is Correct!
The cardiac apex is to the left, the enlarged right border of the heart is due to dilated right atrium due to increased blood flow secondary to atrial septal defect. Ventricular inversion is characterized by apex towards the left as usual, however, the mediastinum is narrow due to abnormal relationship of the great vessels to each other.
Incorrect
Correct answer is D:
The cardiac apex is to the left, the enlarged right border of the heart is due to dilated right atrium due to increased blood flow secondary to atrial septal defect. Ventricular inversion is characterized by apex towards the left as usual, however, the mediastinum is narrow due to abnormal relationship of the great vessels to each other.
Question 20 of 45
20. Question
1 points
Category: CXR in children with heart disease
CXR
In addition to the dextrocardia in this patient, which one of the following findings is noted in the CXR below?
e3
e3
Correct
That is Correct!
The stomach bubble in this patient is leftwards, which is normal. The atrial situs usually follows the abdominal situs, therefore, there is most probably situs solitus. None of the other pathologies are present in this CXR.
Incorrect
Correct answer is A:
The stomach bubble in this patient is leftwards, which is normal. The atrial situs usually follows the abdominal situs, therefore, there is most probably situs solitus. None of the other pathologies are present in this CXR.
Question 21 of 45
21. Question
1 points
Category: CXR in children with heart disease
CXR
What is causing cardiomegaly in the CXR below?
e4
e4
Correct
That is Correct!
Enlarged cardiac silhouette with downwards pointing apex indicates left ventricular hypertrophy. Right ventricular hypertrophy causes upwards lifting of the cardiac apex without enlarging cardiac silhouette in antero-posterior projections of CXR. Right atrial enlargement causes bulging of right heart border, while left atrial enlargement causes widening of carina angle, double left atrial shadow or posterior deviation of esophagus on a lateral projection.
Incorrect
Correct answer is D:
Enlarged cardiac silhouette with downwards pointing apex indicates left ventricular hypertrophy. Right ventricular hypertrophy causes upwards lifting of the cardiac apex without enlarging cardiac silhouette in antero-posterior projections of CXR. Right atrial enlargement causes bulging of right heart border, while left atrial enlargement causes widening of carina angle, double left atrial shadow or posterior deviation of esophagus on a lateral projection.
Question 22 of 45
22. Question
1 points
Category: CXR in children with heart disease
CXR
In what cardiovascular structure is the tip of the central line in this patient?
e5
e5
Correct
That is Correct!
The catheter is placed through internal jugular access and courses through the innominant vein to end in the superior vena cava.
Incorrect
Correct answer is C:
The catheter is placed through internal jugular access and courses through the innominant vein to end in the superior vena cava.
Question 23 of 45
23. Question
1 points
Category: CXR in children with heart disease
CXR
The changes in the CXR below are most probably precipitated by which of the following cardiac lesions:
e6
e6
Correct
That is Correct!
The mediastinum is narrow, which suggests abnormal relationship of the great vessels to each other, this is also seen in atresia of either one of the great vessels.
Incorrect
Correct answer is B:
The mediastinum is narrow, which suggests abnormal relationship of the great vessels to each other, this is also seen in atresia of either one of the great vessels.
Question 24 of 45
24. Question
1 points
Category: CXR in children with heart disease
CXR
Which cardiac lesion is expected in a patient with the CXR below?
e8
e8
Correct
That is correct!
The left ventricle is dilated with slightly prominent pulmonary vascular markings. This patient has rheumatic heart disease with aortic and mitral regurgitation.
Incorrect
Correct answer is C:
The left ventricle is dilated with slightly prominent pulmonary vascular markings. This patient has rheumatic heart disease with aortic and mitral regurgitation.
Question 25 of 45
25. Question
1 points
Category: CXR in children with heart disease
CXR
In addition to cardiomegaly, what abnormality is noted in the CXR below?
e9
e9
Correct
That is Correct!
The pulmonary vascular markings are significantly reduced in this patient with Alagille syndrome with severe peripheral pulmonary stenosis.
Incorrect
Correct answer is A:
The pulmonary vascular markings are significantly reduced in this patient with Alagille syndrome with severe peripheral pulmonary stenosis.
Question 26 of 45
26. Question
1 points
Category: ECG
ECG in pectus excavatum
A 6 year old was seen in the emergency room the previous day for an episode of chest pain. Part of the work up in the ER was a 12 lead ECG, shown below. The parents were told that the child most probably has right ventricular hypertrophy and an appointment with a cardiologist was made. The child is active with no history of easy fatigability or shortness of breath. Past medical and family history are not significant. The child has been complaining of recurrent chest pain over the past 2 weeks with no associated symptoms. There is no history of syncope or palpitation. On examination HR is 90 bpm, regular. RR is 20/min. No cyanosis or pallor is noted. The capillary refill is brisk. No hepatomegaly. No palpable thrill. There is inward deviation of the sternum and chest pain is induced when palpating the right upper edge of the sternum, chest pain induced is described as sharp. First and second heart sounds are normal with a 1-2/6 systolic murmur which is heard in the supine position, but not in the upright position.
f1
f1
Correct
That is Correct!
Pectus excavatum causes the heart to deviate leftwards and clockwise (looking at the heart from the apex) This will cause no hemodynamic effect, however, the change in location of the various cardiac chambers to the fixed position of limb and chest leads will cause the changes in the ECG, this includes the following:
• Negative P wave in V1, because the right atrium becomes more anterior than rightwards.
• RSR’ in V1 as seen with RVH … due to a more anterior position of the RVOT
• QR waves in anterior chest leads … due to a more anterior position of the RV and change of ventricular septal plane.
• Right axis deviation … due to clockwise rotation of the heart.
The chest pain described here is typical of costo-chondritis and is not related to the ECG changes.
Incorrect
Correct answer is D:
Pectus excavatum causes the heart to deviate leftwards and clockwise (looking at the heart from the apex) This will cause no hemodynamic effect, however, the change in location of the various cardiac chambers to the fixed position of limb and chest leads will cause the changes in the ECG, this includes the following:
• Negative P wave in V1, because the right atrium becomes more anterior than rightwards.
• RSR’ in V1 as seen with RVH … due to a more anterior position of the RVOT
• QR waves in anterior chest leads … due to a more anterior position of the RV and change of ventricular septal plane.
• Right axis deviation … due to clockwise rotation of the heart.
The chest pain described here is typical of costo-chondritis and is not related to the ECG changes.
Question 27 of 45
27. Question
1 points
Category: ECG
ECG changes
A 2 year old boy with the following ECG
f2a
At 30 years of age, the ECG is as following:
f2b
f2b
Diagnosis is:
Correct
That is Correct!
The first ECG shows left atrial enlargement (LAE) and left ventricular hypertrophy (LVH). Note that the standardization mark indicates half standard in the chest leads, which means that the R waves in V6 are twice as tall as shown in the ECG. The criterion for LAE is wide and bifid P waves, while LVH is determined by tall R waves in V6 and deep S waves in V1.
The second ECG shows pure R wave in V1 which is indicates right ventricular hypertrophy (RVH); signs of LVH seem to resolve in the second ECG. Therefore, this lesion initially caused LAE and LVH and after several years, LAE and LVH resolved to be replaced by RVH.
Pulmonary stenosis causes RVH and does not impact the left ventricle.
Aortic stenosis on the other hand may cause LVH and even LAE, with prolonged course and severe condition it may lead to pulmonary venous hypertension followed by RVH, however, LVH and LAE should not have resolved.
Patent ductus arteriosus (PDA) causes left to right shunting at the arterial level, resulting in increase pulmonary blood flow and subsequently increase in pulmonary venous return which would cause volume burden on the LA and LV, resulting in the LAE and LVH pattern of the ECG. Years later, the excessive blood flow in the pulmonary circulation will cause pulmonary vascular obstructive disease which would cause less blood flow to the lungs, thus resolution of LAE and LVH and increasing RVH due to developing pulmonary hypertension.
Tetralogy of Fallot causes RVH and does not affect the left heart.
Incorrect
Correct answer is C:
The first ECG shows left atrial enlargement (LAE) and left ventricular hypertrophy (LVH). Note that the standardization mark indicates half standard in the chest leads, which means that the R waves in V6 are twice as tall as shown in the ECG. The criterion for LAE is wide and bifid P waves, while LVH is determined by tall R waves in V6 and deep S waves in V1.
The second ECG shows pure R wave in V1 which is indicates right ventricular hypertrophy (RVH); signs of LVH seem to resolve in the second ECG. Therefore, this lesion initially caused LAE and LVH and after several years, LAE and LVH resolved to be replaced by RVH.
Pulmonary stenosis causes RVH and does not impact the left ventricle.
Aortic stenosis on the other hand may cause LVH and even LAE, with prolonged course and severe condition it may lead to pulmonary venous hypertension followed by RVH, however, LVH and LAE should not have resolved.
Patent ductus arteriosus (PDA) causes left to right shunting at the arterial level, resulting in increase pulmonary blood flow and subsequently increase in pulmonary venous return which would cause volume burden on the LA and LV, resulting in the LAE and LVH pattern of the ECG. Years later, the excessive blood flow in the pulmonary circulation will cause pulmonary vascular obstructive disease which would cause less blood flow to the lungs, thus resolution of LAE and LVH and increasing RVH due to developing pulmonary hypertension.
Tetralogy of Fallot causes RVH and does not affect the left heart.
Question 28 of 45
28. Question
1 points
Category: ECG
ECG
Three year old child presents with the ECG shown below. Capillary refill is brisk with good peripheral pulses and perfusion. What should the first line of therapy be?
f3
f3
Correct
That is Correct!
The rhythm in this ECG is that of atrial flutter. The child is table hemodynamically; therefore, there is no need for cardioversion. Intravenous adenosine push is effective in Supraventricular tachycardia and would not interrupt atrial flutter. Amiodarone is effective in many arrhythmias, atrial flutter included, however, it is not the first line of therapy since it has many side effects such as hypothyroidism and pulmonary fibrosis.
Incorrect
Correct answer is D:
The rhythm in this ECG is that of atrial flutter. The child is table hemodynamically; therefore, there is no need for cardioversion. Intravenous adenosine push is effective in Supraventricular tachycardia and would not interrupt atrial flutter. Amiodarone is effective in many arrhythmias, atrial flutter included, however, it is not the first line of therapy since it has many side effects such as hypothyroidism and pulmonary fibrosis.
Question 29 of 45
29. Question
1 points
Category: ECG
ECG
What is the heart rhythm in the following ECG of a 10 year old boy?
f4
f4
Correct
That is Correct!
There are no p waves in this ECG; therefore, the rhythm is of Junctional origin. The determining factor for differentiating between the first three rhythms is the heart rate. Junctional ectopic tachycardia is a rapid heart rate, noted post0operatively leading to hemodynamic compromise. Accelerated Junctional rhythm is slower and does not cause hemodynamic compromise. The faster Junctional rhythm in the latter two causes the sinus node to be dormant. Escape Junctional rhythm is slow. It occurs with abnormality of the sinus node, resulting in an escape rhythm.
Incorrect
Correct answer is C:
There are no p waves in this ECG; therefore, the rhythm is of Junctional origin. The determining factor for differentiating between the first three rhythms is the heart rate. Junctional ectopic tachycardia is a rapid heart rate, noted post0operatively leading to hemodynamic compromise. Accelerated Junctional rhythm is slower and does not cause hemodynamic compromise. The faster Junctional rhythm in the latter two causes the sinus node to be dormant. Escape Junctional rhythm is slow. It occurs with abnormality of the sinus node, resulting in an escape rhythm.
Question 30 of 45
30. Question
1 points
Category: ECG
ECG
f5
f5
Which one of the following statements describes this ECG correctly?
Correct
That is Correct!
Flutter waves are best seen in leads III and aVF. AV conduction is blocked 2:1
Incorrect
Correct answer is D:
Flutter waves are best seen in leads III and aVF. AV conduction is blocked 2:1
Question 31 of 45
31. Question
1 points
Category: ECG
What is the heart rhythm?
f6
f6
Correct
That is Correct!
The QRS complexes are narrow, indicating a Supraventricular rhythm. No p waves are seen prior to QRS complexes, suggestive of Junctional rhythm.
Incorrect
Correct answer is B:
The QRS complexes are narrow, indicating a Supraventricular rhythm. No p waves are seen prior to QRS complexes, suggestive of Junctional rhythm.
Question 32 of 45
32. Question
1 points
Category: ECG
Which of the following descriptions of atrio-ventricular conduction is accurate?
f7
f7
Correct
That is Correct!
The QRS complexes are wide with RsR pattern in left chest leads (V6), indicative of left bundle branch block.
Incorrect
Correct answer is A:
The QRS complexes are wide with RsR pattern in left chest leads (V6), indicative of left bundle branch block.
Question 33 of 45
33. Question
1 points
Category: ECG
Which of the following diagnosis is most likely in a 5 year old with the above ECG?
f8
f8
Correct
That is Correct!
There is increase in the left ventricular forces (tall R in V6 and deep S in V1) which are indicative of left ventricular hypertrophy, as seen in aortic stenosis. Pulmonary stenosis, tetralogy of Fallot and atrial septal defect all cause right ventricular hypertrophy. Patients with atrial septal defect also have right atrial enlargement.
Incorrect
Correct answer is B:
There is increase in the left ventricular forces (tall R in V6 and deep S in V1) which are indicative of left ventricular hypertrophy, as seen in aortic stenosis. Pulmonary stenosis, tetralogy of Fallot and atrial septal defect all cause right ventricular hypertrophy. Patients with atrial septal defect also have right atrial enlargement.
Question 34 of 45
34. Question
1 points
Category: ECG
ECG
What is wrong with this electrocardiogram?
f9
f9
Correct
That is Correct!
Options B, C and D are correct if they where isolated findings, however, seeing all these abnormalities on ECG suggest that the lead connections are wrong (connecting right leads to left extremities and left leads to right extremities). With this lead connection, the p and QRS axis become abnormal (this ECG suggest low left atrial axis which is very unusual). In addition q waves are seen in leads which should not have any q waves such leads I and aVL.
Incorrect
Correct answer is A:
Options B, C and D are correct if they where isolated findings, however, seeing all these abnormalities on ECG suggest that the lead connections are wrong (connecting right leads to left extremities and left leads to right extremities). With this lead connection, the p and QRS axis become abnormal (this ECG suggest low left atrial axis which is very unusual). In addition q waves are seen in leads which should not have any q waves such leads I and aVL.
Question 35 of 45
35. Question
1 points
Category: ECG
ECG
Which of the following options is most likely consistent with the ECG here?
f10
f10
Correct
That is Correct!
The ECG is normal; option C suggests an innocent heart murmur. Option A suggests a ventricular septal defect which would likely have LVH and possibly RVH. Option B suggests mitral stenosis, which would have left atrial enlargement. Option D suggests pulmonary hypertension which would be associated with right ventricular hypertrophy.
Incorrect
Correct answer is C:
The ECG is normal; option C suggests an innocent heart murmur. Option A suggests a ventricular septal defect which would likely have LVH and possibly RVH. Option B suggests mitral stenosis, which would have left atrial enlargement. Option D suggests pulmonary hypertension which would be associated with right ventricular hypertrophy.
Question 36 of 45
36. Question
1 points
Category: ECG
ECG
f11
f11
Which of the following rhythms best describe the ECG in this question?
Correct
That is Correct!
The rhythm is sinus with occasional wide QRS complexes not proceeded by a p wave indicating premature ventricular contraction.
Incorrect
Correct answer is C:
The rhythm is sinus with occasional wide QRS complexes not proceeded by a p wave indicating premature ventricular contraction.
Question 37 of 45
37. Question
1 points
Category: ECG
ECG
f12
f12
Which of the following best describes the ECG in this question?
Correct
That is Correct!
The giant P waves suggest Ebstein’s malformation.
Incorrect
Correct answer is B:
The giant P waves suggest Ebstein’s malformation.
Question 38 of 45
38. Question
1 points
Category: ECG
ECG
f13
f13
Which one of the following auscultatory findings would you expect a 4 year old with the above ECG to have?
Correct
That is Correct!
Murmur in case scenario (A) is consistent with ventricular septal defect, the holosystolic murmur is caused by left to right shunting at the defect, while the mid-diastolic murmur is due to increase flow across the mitral valve.
Murmur in scenario (B) is typical of an atrial septal defect. The systolic murmur is due to increase blood flow across the pulmonary valve, while the diastolic murmur is due to increase flow across the tricuspid valve. Fixed splitting of S2 is due to constant delay of pulmonary valve closure due to increase flow across the pulmonary valve due to left to right shunting at the atrial septal defect.
Murmur in scenario (C) is consistent with a patent ductus arteriosus. The cause of the clicking noise is not clear, but observed in these patients, thus the description “machinery murmur”.
Murmur in scenario (D) is consistent with mitral valve prolapse.
Incorrect
Correct answer is B:
Murmur in case scenario (A) is consistent with ventricular septal defect, the holosystolic murmur is caused by left to right shunting at the defect, while the mid-diastolic murmur is due to increase flow across the mitral valve.
Murmur in scenario (B) is typical of an atrial septal defect. The systolic murmur is due to increase blood flow across the pulmonary valve, while the diastolic murmur is due to increase flow across the tricuspid valve. Fixed splitting of S2 is due to constant delay of pulmonary valve closure due to increase flow across the pulmonary valve due to left to right shunting at the atrial septal defect.
Murmur in scenario (C) is consistent with a patent ductus arteriosus. The cause of the clicking noise is not clear, but observed in these patients, thus the description “machinery murmur”.
Murmur in scenario (D) is consistent with mitral valve prolapse.
Question 39 of 45
39. Question
1 points
Category: ECG
ECG
f14
f14
Which of the following statements best describe the atrio-ventricular conduction in this ECG?
Correct
That is Correct!
The QRS complexes are wide with RsR pattern in right chest leads (V1), indicative of right bundle branch block.
Incorrect
Correct answer is C:
The QRS complexes are wide with RsR pattern in right chest leads (V1), indicative of right bundle branch block.
Question 40 of 45
40. Question
1 points
Category: ECG
ECG
f15
f15
Which one of the following statements best describe the most likely cause of the qr pattern of QRS complex in lead V1?
Correct
That is Correct!
qr pattern of QRS complex in the right chest lead is indicative of any of the above mentioned causes, it is also found in pectus excavatum. RVH is most likely in this ECG in view of normal QRS axis (80 degrees). All other cases would most probably have abnormal QRS axis.
Incorrect
Correct answer is D:
qr pattern of QRS complex in the right chest lead is indicative of any of the above mentioned causes, it is also found in pectus excavatum. RVH is most likely in this ECG in view of normal QRS axis (80 degrees). All other cases would most probably have abnormal QRS axis.
Question 41 of 45
41. Question
1 points
Category: ECG
ECG
f16
f16
Which of the following statements best describe the rhythm in this ECG?
Correct
That is Correct!
The rhythm is sinus (normal axis p waves preceding each QRS complex). The p wave rate changes with respiration, thus consistent with sinus arrhythmia. In Wenckebach the PR interval becomes progressively longer, then a p wave does not conduct.
Incorrect
Correct answer is A:
The rhythm is sinus (normal axis p waves preceding each QRS complex). The p wave rate changes with respiration, thus consistent with sinus arrhythmia. In Wenckebach the PR interval becomes progressively longer, then a p wave does not conduct.
Question 42 of 45
42. Question
1 points
Category: ECG
ECG
f17
f17
What is concerning in this ECG in a 6 month old?
Correct
That is Correct!
The heart rate (60 bpm) is too slow for a 6 month old. This is sinus bradycardia.
Incorrect
Correct answer is A:
The heart rate (60 bpm) is too slow for a 6 month old. This is sinus bradycardia.
Question 43 of 45
43. Question
1 points
Category: ECG
ECG
f18
f18
What is the first line of treatment in a 6 month (with the ECG shown) who is alert, in no distress and capillary refill of 2 seconds?
Correct
That is Correct!
The child should be cardioverted if hemodynamically unstable, which is not the case in this example. Amiodarone orally requires several days to be effective. Vagal stimulation could be attempted here, but not through pressure over eyeballs, which is contraindicated in young children as damage to the eyeball may result.
Incorrect
Correct answer is B:
The child should be cardioverted if hemodynamically unstable, which is not the case in this example. Amiodarone orally requires several days to be effective. Vagal stimulation could be attempted here, but not through pressure over eyeballs, which is contraindicated in young children as damage to the eyeball may result.
Question 44 of 45
44. Question
1 points
Category: ECG
ECG
f19
f19
When is it acceptable to give adenosine in a patient with the rhythm presented in this ECG?
Correct
That is Correct!
The rhythm in this ECG shows wide QRS complex tachycardia. Treatment in this case should be initially fashioned as if the abnormal rhythm is ventricular tachycardia. However, in the presence of known bundle branch block with similar pattern QRS as before the arrhythmia, then the rapid heart rate in this case may be secondary to Supraventricular tachycardia and treatment with adenosine could be considered.
Incorrect
Correct answer is C:
The rhythm in this ECG shows wide QRS complex tachycardia. Treatment in this case should be initially fashioned as if the abnormal rhythm is ventricular tachycardia. However, in the presence of known bundle branch block with similar pattern QRS as before the arrhythmia, then the rapid heart rate in this case may be secondary to Supraventricular tachycardia and treatment with adenosine could be considered.
Question 45 of 45
45. Question
1 points
Category: ECG
ECG
f20
f20
The cause for wide QRS in this ECG is related to which one of the following factors?
Correct
That is Correct!
This ECG demonstrates short pr interval with delta waves (causing wide QRS) in inferior and lateral chest leads. These findings are consistent with Wolf-Parkinson-White syndrome.
Incorrect
Correct answer is A:
This ECG demonstrates short pr interval with delta waves (causing wide QRS) in inferior and lateral chest leads. These findings are consistent with Wolf-Parkinson-White syndrome.
Time limit: 0
Quiz-summary
0 of 51 questions completed
Questions:
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
Information
CCHD Exam – Part III
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You must sign in or sign up to start the quiz.
You have to finish following quiz, to start this quiz:
Results
0 of 51 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 points, (0)
Average score
Your score
Categories
Cardiac catheterization and therapeutic catheterization0%
Congenital heart disease0%
Echocardiography0%
Operative therapy for heart diseases in children0%
Post-operative care in children with heart disease0%
Congratulations on a job well done!
Your result has been entered into leaderboard
Loading
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
Answered
Review
Question 1 of 51
1. Question
1 points
Category: Echocardiography
Echo
Side effects of echocardiography when used in a one year old child 2 days after surgical repair of ventricular septal defect include which one of the following?
Correct
Correct !
Echocardiography is safe to use in children. It utilizes ultrasound waves, which are harmless to human tissue. Continuous wave Doppler may cause increase in body temperature when used for prolonged periods in premature infants with small body mass. Ultrasound waves are not known to interfere with wound healing. The only precaution needed in the post-operative period is the use of sterile technique so as not to cause wound infection.
Incorrect
Correct answer is D
Echocardiography is safe to use in children. It utilizes ultrasound waves, which are harmless to human tissue. Continuous wave Doppler may cause increase in body temperature when used for prolonged periods in premature infants with small body mass. Ultrasound waves are not known to interfere with wound healing. The only precaution needed in the post-operative period is the use of sterile technique so as not to cause wound infection.
Question 2 of 51
2. Question
1 points
Category: Cardiac catheterization and therapeutic catheterization
Cath
Patient with the following lesions should all undergo cardiac catheterization except one. Choose the one lesion from below which does not need cardiac catheterization.
Correct
Correct !
Cardiac catheterization is performed for 2 reasons: 1) Obtain diagnostic data such as pressures and magnitude of shunt lesions, or 2) Provide therapeutic measures such as close defects or reduce pressure gradients of stenotic valves and vessels.
A small mid-muscular VSD is hemodynamically insignificant and does not pose threat to cardiac valves as some outflow ventricular septal defects do. Therefore closure with a device, such as the Amplatz device is not necessary.
A large secundum atrial septal defect is hemodynamically significant and will not close spontaneously; therefore, closure in the catheterization laboratory is indicated.
Patent ductus arteriosus should be closed at all ages outside the neonatal period since it poses high bacterial endocarditis risk. Most cardiologists advocate observation only of small patent ductus arteriosus not associated with a murmur (silent), since the risk of bacterial endocarditis is negligible in such lesions.
Incorrect
Correct answer is C:
Cardiac catheterization is performed for 2 reasons: 1) Obtain diagnostic data such as pressures and magnitude of shunt lesions, or 2) Provide therapeutic measures such as close defects or reduce pressure gradients of stenotic valves and vessels.
A small mid-muscular VSD is hemodynamically insignificant and does not pose threat to cardiac valves as some outflow ventricular septal defects do. Therefore closure with a device, such as the Amplatz device is not necessary.
A large secundum atrial septal defect is hemodynamically significant and will not close spontaneously; therefore, closure in the catheterization laboratory is indicated.
Patent ductus arteriosus should be closed at all ages outside the neonatal period since it poses high bacterial endocarditis risk. Most cardiologists advocate observation only of small patent ductus arteriosus not associated with a murmur (silent), since the risk of bacterial endocarditis is negligible in such lesions.
Question 3 of 51
3. Question
1 points
Category: Cardiac catheterization and therapeutic catheterization
Cath
All the following lesions are amenable to therapeutic intervention in the cardiac catheterization laboratory except one. Identify the lesion which should not be considered for interventional cardiac catheterization:
Correct
Correct !
Secundum atrial septal defect can be closed by occlusion devices as long as there is a reasonable rim of atrial septal tissue surrounding the defect to enable anchoring of device.
Apical ventricular septal defects are difficult to close surgically sine the area is not easily accessible to the surgeon without a left ventriculotomy which may leave the left ventricle scarred.
Sinus venosus atrial septal defects lack a rim of tissue adjacent to the superior and/or inferior vena cava and such are not amenable to device closure in the catheterization laboratory.
Pulmonary stenosis in patients with atrial septal defects restrict blood flow to the lungs and thus prevent significant congestive heart failure, however the combination of these two lesions result in right ventricular volume and pressure overload. Both lesions can be treated in the catheterization laboratory in one setting.
Incorrect
Correct answer is C:
Secundum atrial septal defect can be closed by occlusion devices as long as there is a reasonable rim of atrial septal tissue surrounding the defect to enable anchoring of device.
Apical ventricular septal defects are difficult to close surgically sine the area is not easily accessible to the surgeon without a left ventriculotomy which may leave the left ventricle scarred.
Sinus venosus atrial septal defects lack a rim of tissue adjacent to the superior and/or inferior vena cava and such are not amenable to device closure in the catheterization laboratory.
Pulmonary stenosis in patients with atrial septal defects restrict blood flow to the lungs and thus prevent significant congestive heart failure, however the combination of these two lesions result in right ventricular volume and pressure overload. Both lesions can be treated in the catheterization laboratory in one setting.
Question 4 of 51
4. Question
1 points
Category: Cardiac catheterization and therapeutic catheterization
Cath
A chest x-ray obtained 3 hours after an interventional procedure to close an atrial septal defect was obtained. The cardiac silhouette is much larger than previously noted. The heart sounds are muffled with no murmur by auscultation. Peripheral pulses are diminished. The likely cause of this clinical picture is:
Correct
Correct !
The clinical picture is consistent with pericardial effusion and pending tamponade. This may be a result of trauma to cardiovascular walls during catheterization by catheters or the occlusion device. A large residual atrial septal defect will not cause any more congestive heart failure than before device closure, therefore unlikely to cause this picture of poor cardiac output.
Cardiac arrhythmia may occur during the catheterization procedure and occasionally persists thereafter; however, this will not lead to large cardiac silhouette or muffled cardiac tones.
Allergic reaction may manifest after contrast injection such as skin manifestation, upper airway obstruction, etc. This patient did not present with these manifestations.
Incorrect
Correct answer is B:
The clinical picture is consistent with pericardial effusion and pending tamponade. This may be a result of trauma to cardiovascular walls during catheterization by catheters or the occlusion device. A large residual atrial septal defect will not cause any more congestive heart failure than before device closure, therefore unlikely to cause this picture of poor cardiac output.
Cardiac arrhythmia may occur during the catheterization procedure and occasionally persists thereafter; however, this will not lead to large cardiac silhouette or muffled cardiac tones.
Allergic reaction may manifest after contrast injection such as skin manifestation, upper airway obstruction, etc. This patient did not present with these manifestations.
Question 5 of 51
5. Question
1 points
Category: Operative therapy for heart diseases in children
CHD surgery
A 6 month old with Tetralogy of Fallot has an oxygen saturation of 85%. There is no history of hypercyanotic spells. Which of the following statements is correct regarding surgical correction?
Correct
Correct !
Complete surgical repair in all patients with Tetralogy of Fallot should be considered when the child is 6 months of age since the morbidity and mortality of complete surgical repair plateaus after 6 months of age. Complete repair should not be delayed, if possible, beyond 1 year of age as the risk of brain abscess or embolization due to right to left shunting at the ventricular septal defect increases after the first year of age. A systemic to pulmonary arterial shunt is used only when complete surgical repair is not possible due to small pulmonary branches or unstable patients. Complete surgical repair entails closure of ventricular septal defect with a patch, enlarging the right ventricular outflow through muscle resection and patch placement. Pulmonary valve annulus is best left without patch placement if near normal in size, however if small it could be enlarged with a patch. Patch enlargement of the pulmonary valve annulus will eliminate pulmonary valve stenosis, but at the expense of significant pulmonary regurgitation which will eventually lead to right ventricular dilation and dysfunction and arrhythmias. Down syndrome has no impact on timing of surgery as it does not reduce or increase operative risks.
Incorrect
Correct answer is A:
Complete surgical repair in all patients with Tetralogy of Fallot should be considered when the child is 6 months of age since the morbidity and mortality of complete surgical repair plateaus after 6 months of age. Complete repair should not be delayed, if possible, beyond 1 year of age as the risk of brain abscess or embolization due to right to left shunting at the ventricular septal defect increases after the first year of age. A systemic to pulmonary arterial shunt is used only when complete surgical repair is not possible due to small pulmonary branches or unstable patients. Complete surgical repair entails closure of ventricular septal defect with a patch, enlarging the right ventricular outflow through muscle resection and patch placement. Pulmonary valve annulus is best left without patch placement if near normal in size, however if small it could be enlarged with a patch. Patch enlargement of the pulmonary valve annulus will eliminate pulmonary valve stenosis, but at the expense of significant pulmonary regurgitation which will eventually lead to right ventricular dilation and dysfunction and arrhythmias. Down syndrome has no impact on timing of surgery as it does not reduce or increase operative risks.
Question 6 of 51
6. Question
1 points
Category: Operative therapy for heart diseases in children
CHD surgery
Surgical closure of an atrial septal defect should be first choice of therapy in a 5 year old child in all the following types of atrial septal defect, except one. Which one of the following defects should be considered for cardiac catheterization device closure rather than surgery?
Correct
Correct !
Only secundum atrial septal defect could be closed by device as it requires atrial septal wall surrounding the defect which is not present in primum and sinus venosus type atrial septal defects. Pulmonary valve stenosis could be treated in the catheterization laboratory by balloon dilation at the same time an atrial septal defect device is deployed.
Incorrect
Correct answer is D:
Only secundum atrial septal defect could be closed by device as it requires atrial septal wall surrounding the defect which is not present in primum and sinus venosus type atrial septal defects. Pulmonary valve stenosis could be treated in the catheterization laboratory by balloon dilation at the same time an atrial septal defect device is deployed.
Question 7 of 51
7. Question
1 points
Category: Operative therapy for heart diseases in children
CHD surgery
What is the sequence of surgical procedures required for a newborn with tricuspid atresia and large patent ductus arteriosus?
Correct
Correct !
A child with tricuspid atresia is dependent upon the patent ductus arteriosus for pulmonary blood flow. Therefore, prostaglandin infusion is important soon after diagnosis. Once the child is stable, 1-2 weeks of age, a systemic to pulmonary arterial shunt will provide a reliable source of pulmonary blood flow without the disadvantages of prostaglandin infusion. A Glenn shunt connects the superior vena cava directly to the right pulmonary artery; this cannot be done prior 6-9 months of age since the normally elevated pulmonary vascular resistance does not allow proper function of a Glenn shunt which requires low pulmonary vascular resistance for proper functioning. A Glenn shunt should maintain the oxygen saturation at about 80% till the child is about 18-24 months of age, at which time a Fontan procedure could be performed. Fontan procedure entails connecting the inferior vena cava to the pulmonary arteries through a tunnel within the right atrium or an extra-cardiac conduit. The Fontan procedure allows all systemic venous return (except that from the coronary sinus) to flow directly to the pulmonary circulation, bypassing the cardiac chambers.
Incorrect
Correct answer is D:
A child with tricuspid atresia is dependent upon the patent ductus arteriosus for pulmonary blood flow. Therefore, prostaglandin infusion is important soon after diagnosis. Once the child is stable, 1-2 weeks of age, a systemic to pulmonary arterial shunt will provide a reliable source of pulmonary blood flow without the disadvantages of prostaglandin infusion. A Glenn shunt connects the superior vena cava directly to the right pulmonary artery; this cannot be done prior 6-9 months of age since the normally elevated pulmonary vascular resistance does not allow proper function of a Glenn shunt which requires low pulmonary vascular resistance for proper functioning. A Glenn shunt should maintain the oxygen saturation at about 80% till the child is about 18-24 months of age, at which time a Fontan procedure could be performed. Fontan procedure entails connecting the inferior vena cava to the pulmonary arteries through a tunnel within the right atrium or an extra-cardiac conduit. The Fontan procedure allows all systemic venous return (except that from the coronary sinus) to flow directly to the pulmonary circulation, bypassing the cardiac chambers.
Question 8 of 51
8. Question
1 points
Category: Operative therapy for heart diseases in children
CHD surgery
All the following cardiac conditions can be maintained without surgery in the neonatal period, except one condition which presents in an emergency fashion in the neonatal period requiring surgical intervention. Which of the following congenital heart diseases require urgent surgical intervention in the neonatal period?
Correct
Correct !
When all pulmonary veins drain in an anomalous fashion to the superior vena cava, the connecting veins are typical small and may become stenosed resulting in severe obstruction. Therefore, such children are repaired immediately. Large apical ventricular septal defect may cause congestive heart failure which does not respond to medications, however, this typically occurs at few weeks of age. Large apical ventricular septal defect could be closed by a device in the cardiac catheterization laboratory or palliated by placing a band on the pulmonary artery to restrict blood flow.
Double outlet right ventricle and transposition of the great vessels with large atrial and ventricular septal defects are stable lesions which result in mild to moderate oxygen desaturation, thus allowing the child to grow for few weeks to months prior to the need to surgically intervene.
Incorrect
Correct answer is A:
When all pulmonary veins drain in an anomalous fashion to the superior vena cava, the connecting veins are typical small and may become stenosed resulting in severe obstruction. Therefore, such children are repaired immediately. Large apical ventricular septal defect may cause congestive heart failure which does not respond to medications, however, this typically occurs at few weeks of age. Large apical ventricular septal defect could be closed by a device in the cardiac catheterization laboratory or palliated by placing a band on the pulmonary artery to restrict blood flow.
Double outlet right ventricle and transposition of the great vessels with large atrial and ventricular septal defects are stable lesions which result in mild to moderate oxygen desaturation, thus allowing the child to grow for few weeks to months prior to the need to surgically intervene.
Question 9 of 51
9. Question
1 points
Category: Operative therapy for heart diseases in children
CHD surgery
Surgery should be delayed in a 2 year old with large ventricular septal defect in all the following scenarios except one. Which of the following added complication is not a contraindication to surgical repair?
Correct
Correct !
Pulmonary edema is the result of large pulmonary blood flow secondary to left to right shunting at the ventricular septal defect. Surgical repair will cure this.
Sepsis or recent RSV pneumonitis are contraindications to surgery since the immune system is depressed secondary to surgical intervention due to the cardio-pulmonary by-pass machine. Cardiac surgery requires heparinaztion which will be deleterious to a child with cerebral hemorrhage.
Incorrect
Correct answer is B:
Pulmonary edema is the result of large pulmonary blood flow secondary to left to right shunting at the ventricular septal defect. Surgical repair will cure this.
Sepsis or recent RSV pneumonitis are contraindications to surgery since the immune system is depressed secondary to surgical intervention due to the cardio-pulmonary by-pass machine. Cardiac surgery requires heparinaztion which will be deleterious to a child with cerebral hemorrhage.
Question 10 of 51
10. Question
1 points
Category: Post-operative care in children with heart disease
Diuretics in post-operative care
An 8 month old infant is in the cardiac intensive care unit 2 days after surgical closure of a large ventricular septal defect. There is a concern that the urine output has diminished over the past 12 hours. Vital signs are as following: heart rate is 165 bpm, central venous pressure is 2 mmHg, blood pressure is 85/65 mmHg, and oxygen saturation is 97%.
Review of fluid intake and output over the past 2 days show the following: input was 85 cc/kg the preceding day and 90 cc/kg the day before, while urine output 5 cc/kg/hour the previous 2days. Child’s weight is 7 kg.
Serum electrolytes are as following: sodium 137 mEq/l, potassium 3 mEq/l, chloride is 98 mEq/l, bicarbonate 20 mEq/l. BUN is 30 mg/dl.
The medications currently used are:
Milrinone 7 mcg/kg/min intravenous infusion
Furosemide 10 mg/kg intravenously every 6 hours
Which of the following actions is indicated in this patient?
j6
j6
Correct
Correct !
This drop in the urine output in this child is most probably secondary to excessive diuresis over the past 2 days due to aggressive furosemide dosing. This is supported by a low central venous pressure and elevated BUN. It is not necessary to add new pharmacologic agents or infuse with fluid. Withholding furosemide or adjusting to a lower dose will most probably correct the anomaly.
Incorrect
Correct answer is B:
This drop in the urine output in this child is most probably secondary to excessive diuresis over the past 2 days due to aggressive furosemide dosing. This is supported by a low central venous pressure and elevated BUN. It is not necessary to add new pharmacologic agents or infuse with fluid. Withholding furosemide or adjusting to a lower dose will most probably correct the anomaly.
Question 11 of 51
11. Question
1 points
Category: Congenital heart disease
VSD 2
In a 3 year old boy with a ventricular septal defect (VSD), which one of the following scenarios will make the VSD more likely to spontaneously close?
Correct
That is Correct!
Perimembranous VSD tend to close by incorporation of tricuspid valve tissue. This forms an aneurysmal pouch at its orifice, which is likely to eventually completely close the VSD defect.
Option A is incorrect since large muscular VSDs, including those in the apex are not likely to spontaneously close.
Option B is incorrect since outflow tract VSDs are less likely to spontaneously close than perimembranous or muscular VSDs.
Option D is incorrect since inlet VSD with or without AVCD does not close spontaneously.
Incorrect
Correct answer is C:
Perimembranous VSD tend to close by incorporation of tricuspid valve tissue. This forms an aneurysmal pouch at its orifice, which is likely to eventually completely close the VSD defect.
Option A is incorrect since large muscular VSDs, including those in the apex are not likely to spontaneously close.
Option B is incorrect since outflow tract VSDs are less likely to spontaneously close than perimembranous or muscular VSDs.
Option D is incorrect since inlet VSD with or without AVCD does not close spontaneously.
Question 12 of 51
12. Question
1 points
Category: Congenital heart disease
PDA 1
A 5 year old is known to have a patent ductus arteriosus (PDA). Previous echocardiographic assessments documented a small PDA with restrictive left to right shunting. History reveals a healthy growing child with no evidence of easy fatigability or shortness of breath. Recent chest x-ray and electrocardiograms are within normal limits. The pediatric cardiologist involved in the care of this child is recommending per-catheter closure of the PDA even though it is hemodynamically insignificant. Which of the following statemtns accurately states the reason for this recommendation?
Correct
That is Correct!
PDA is known to pose a higher risk of sub-acute bacterial endocarditis than other lesions, possibly due to the high terbulent flow. All PDAs should be closed. Attempts to close in the cardiac catheterization laboratory should be attempted first, if not possible, then surgical closure is recommended.
Congestive heart failure in patients with PDA is related to the amount of blood flow shunted across. Small defects should cause limited increase in pulmonary blood flow and consequently not cause congestive heart failure.
Pulmonary vascular obstructive disease is not expected as a complication to a small PDA due to limited increase in pulmonary blood flow with no significant impact on pulmonary vasculature.
Paradoxical embolization is known to occur with small atrial septal defects or even patent foramen ovale, but not with PDA.
Incorrect
Correct answer is B:
PDA is known to pose a higher risk of sub-acute bacterial endocarditis than other lesions, possibly due to the high terbulent flow. All PDAs should be closed. Attempts to close in the cardiac catheterization laboratory should be attempted first, if not possible, then surgical closure is recommended.
Congestive heart failure in patients with PDA is related to the amount of blood flow shunted across. Small defects should cause limited increase in pulmonary blood flow and consequently not cause congestive heart failure.
Pulmonary vascular obstructive disease is not expected as a complication to a small PDA due to limited increase in pulmonary blood flow with no significant impact on pulmonary vasculature.
Paradoxical embolization is known to occur with small atrial septal defects or even patent foramen ovale, but not with PDA.
Question 13 of 51
13. Question
1 points
Category: Congenital heart disease
AVCD 2
During follow up of a 6month old with complete atrioventricular canal defect and normal chromosomal pattern is noted to have oxygen saturation of 90% by pulse oximetry. The child is failing to thrive. Auscultation is significant for a 3/6 holosystolic murmur at the apical region. Chest x-ray shows cardiomegaly and increase pulmonary blood flow. What is the cause of the low oxygen saturation?
Correct
Correct !
This child with complete atrioventricular canal defect has evidence of large shunting (at atrial and ventricular levels) causing increase pulmonary blood flow and congestive heart failure. Patients with complete atrioventricular canal defects may have large atrial and ventricular level defects allowing for some mixing of blood and mild desaturation as in this case. Oxygen desaturation due to high pulmonary vascular resistance is unlikely at 6 months of age, particularly in a patient without Down syndrome. Furthermore, elevated pulmonary vascular resistance resulting in pulmonary hypertension will have reduced pulmonary blood flow, not increased as it is clear in this case. Pulmonary stenosis, or tetralogy of Fallot when combined with complete atrioventricular canal defect present with cyanosis, but again these patients do not have evidence of increased pulmonary blood flow.
Incorrect
Correct answer is C:
This child with complete atrioventricular canal defect has evidence of large shunting (at atrial and ventricular levels) causing increase pulmonary blood flow and congestive heart failure. Patients with complete atrioventricular canal defects may have large atrial and ventricular level defects allowing for some mixing of blood and mild desaturation as in this case. Oxygen desaturation due to high pulmonary vascular resistance is unlikely at 6 months of age, particularly in a patient without Down syndrome. Furthermore, elevated pulmonary vascular resistance resulting in pulmonary hypertension will have reduced pulmonary blood flow, not increased as it is clear in this case. Pulmonary stenosis, or tetralogy of Fallot when combined with complete atrioventricular canal defect present with cyanosis, but again these patients do not have evidence of increased pulmonary blood flow.
Question 14 of 51
14. Question
1 points
Category: Congenital heart disease
Truncus arteriosus
When planning surgical repair of a newborn with tetralogy of Fallot and pulmonary atresia, initially a shunt is placed from the systemic to pulmonary arterial circulation to secure pulmonary blood flow. This is followed by complete repair at about 6 months of age where the shunt is taken down and a homograft is placed between the right ventricle and pulmonary arteries with closure of the ventricular septal defect. On the other hand, newborns with truncus arteriosus it is customary to plan for complete surgical repair within the first 2 weeks of life. In this repair, the ventricular septal defect is closed with separation of the pulmonary artery from the truncus and placement of a homograft from the right ventricle to the pulmonary arteries. Why is complete repair in truncus arteriosus planned early in life in comparison to other lesions, such as tetralogy of Fallot with pulmonary atresia?
Correct
Correct !
In truncus arteriosus the pulmonary arteries are connected directly to the truncus (ascending aorta). The right and left pulmonary arteries may be connected together, through a short main pulmonary artery, or separately. Either way, there is no pulmonary valve. The hallmark of truncus arteriosus is presence of a single semilunar valve. Since the pulmonary arteries are directly connected to the truncus, a ductus arteriosus becomes unnecessary, though sometimes present. The pulmonary arteries tend to be small; however, the direct communication to the aorta results in high pulmonary blood flow and good oxygen saturation as well as resulting in pulmonary edema and congestive heart failure. The high pulmonary blood flow and risk of early pulmonary vascular resistance may result in pulmonary vascular obstructive disease, thus necessitating early surgical repair.
Incorrect
Correct answer is A:
In truncus arteriosus the pulmonary arteries are connected directly to the truncus (ascending aorta). The right and left pulmonary arteries may be connected together, through a short main pulmonary artery, or separately. Either way, there is no pulmonary valve. The hallmark of truncus arteriosus is presence of a single semilunar valve. Since the pulmonary arteries are directly connected to the truncus, a ductus arteriosus becomes unnecessary, though sometimes present. The pulmonary arteries tend to be small; however, the direct communication to the aorta results in high pulmonary blood flow and good oxygen saturation as well as resulting in pulmonary edema and congestive heart failure. The high pulmonary blood flow and risk of early pulmonary vascular resistance may result in pulmonary vascular obstructive disease, thus necessitating early surgical repair.
Question 15 of 51
15. Question
1 points
Category: Congenital heart disease
Which of the following cardiac conditions is NOT likely to cause sudden death?
Correct
Correct !
The left coronary artery tends to be the dominant coronary artery. Coursing between the two great vessels due to an anomalous origin is likely to cause sudden death. On the other hand, anomalous origin of the right coronary artery is not known to cause sudden death. Both idiopathic hypertrophic sub-aortic stenosis and prolonged QT syndrome may cause sudden death, the former due to sudden obstruction of an already small left ventricular outflow tract and the latter due to the potential to develop ventricular tachycardia (torsades de pointis).
Incorrect
Correct answer is B:
The left coronary artery tends to be the dominant coronary artery. Coursing between the two great vessels due to an anomalous origin is likely to cause sudden death. On the other hand, anomalous origin of the right coronary artery is not known to cause sudden death. Both idiopathic hypertrophic sub-aortic stenosis and prolonged QT syndrome may cause sudden death, the former due to sudden obstruction of an already small left ventricular outflow tract and the latter due to the potential to develop ventricular tachycardia (torsades de pointis).
Question 16 of 51
16. Question
1 points
Category: Echocardiography
Echo
A 4 year old girl admitted to the intensive care unit with fever and lethargy. �She is known to have small ventricular septal defect. �Heart rate is 140 bpm, regular, respiratory rate is 40/minute. �Blood pressure is 60/50 mmHg. �Skin color is pale and ashen, mild to moderate respiratory distress is noted. �There is no clubbing of digits or hepatomegaly. �Capillary refill is 3-4 seconds. �Auscultation reveals a harsh 3/6 holosystolic murmur heard best at the left lower sternal border and a 2/4 early diastolic murmur at the right upper sternal border.
What would the shortening fraction of the left ventricle, as demonstrated by echocardiography, most likely be in this patient?
Correct
Correct !
A normal shortening fraction of the left ventricle is 28-35%. �A child with cardiogenic shock, as in this case, will have lower shortening fraction.
Incorrect
Correct Answer is A
A normal shortening fraction of the left ventricle is 28-35%. �A child with cardiogenic shock, as in this case, will have lower shortening fraction.
Question 17 of 51
17. Question
1 points
Category: Echocardiography
Echo
Which of the following investigative tests is best in demonstrating vegetations at the tip of a central venous catheter?
Correct
Correct !
2-D echocardiography show cardiac structures well. �Central venous catheters and vegetations are well demonstrated by 2-D echocardiography. �Color Doppler is used to demonstrate blood flow, while Doppler echocardiography demonstrates pressure gradients across cardiac structures. �Chest radiography shows catheters well, but not capable of demonstrating soft tissue such as vegetations within the cardiac silhouette.
Incorrect
Correct answer is D
2-D echocardiography show cardiac structures well. �Central venous catheters and vegetations are well demonstrated by 2-D echocardiography. �Color Doppler is used to demonstrate blood flow, while Doppler echocardiography demonstrates pressure gradients across cardiac structures. �Chest radiography shows catheters well, but not capable of demonstrating soft tissue such as vegetations within the cardiac silhouette.
Question 18 of 51
18. Question
1 points
Category: Echocardiography
Echo
Inability to visualize the heart by echocardiography in a child in the intensive care unit after cardiac surgery may indicate which of the following pathologies?
Correct
Correct !
Ultrasound waves are reflected when it passes from soft tissue to air and as such it cannot penetrate Pneumopericardium. �Accumulation of fluid in the pleura or pericardium does not cause significant ultrasound waves reflection and are very well visualized by echocardiography. �Mediastinitis does not significantly alter ultrasound waves, and as such does not interfere with cardiac imaging.
Incorrect
Correct answer is C
Ultrasound waves are reflected when it passes from soft tissue to air and as such it cannot penetrate Pneumopericardium. �Accumulation of fluid in the pleura or pericardium does not cause significant ultrasound waves reflection and are very well visualized by echocardiography. �Mediastinitis does not significantly alter ultrasound waves, and as such does not interfere with cardiac imaging.
Question 19 of 51
19. Question
1 points
Category: Echocardiography
Echo
Which of the following causes of chest pain can be diagnosed by echocardiography?
Correct
Correct !
Echocardiography is not a sensitive tool in the assessment of chest pain. �However, it can demonstrate one of the rare causes of chest pain: Anomalous left coronary artery from right coronary sinus. �In this abnormality, the left coronary artery emerges in an anomalous fashion from the right coronary sinus, thus coursing between the aorta and pulmonary arterial trunk. �With exercise, this coronary artery may be compressed causing myocardial ischemia or even sudden death.
Incorrect
Correct answer is B
Echocardiography is not a sensitive tool in the assessment of chest pain. �However, it can demonstrate one of the rare causes of chest pain: Anomalous left coronary artery from right coronary sinus. �In this abnormality, the left coronary artery emerges in an anomalous fashion from the right coronary sinus, thus coursing between the aorta and pulmonary arterial trunk. �With exercise, this coronary artery may be compressed causing myocardial ischemia or even sudden death.
Question 20 of 51
20. Question
1 points
Category: Cardiac catheterization and therapeutic catheterization
Cath
Which of the following lesions is better demonstrated by cardiac catheterization versus transthoracic echocardiography?
Correct
Correct !
Cardiac valves and structures are seen well with echocardiography since it shows soft tissue well. �On the other hand peripheral pulmonary vascular tree is within lung tissues which act as a barrier to ultrasound waves.
Incorrect
Correct answer is A:
Cardiac valves and structures are seen well with echocardiography since it shows soft tissue well. �On the other hand peripheral pulmonary vascular tree is within lung tissues which act as a barrier to ultrasound waves.
Question 21 of 51
21. Question
1 points
Category: Cardiac catheterization and therapeutic catheterization
Cath
How the shunt volume of an atrial septal defect is typically measured in the catheterization laboratory?
Correct
Correct !
Atrial septal defect shunt is best measured by comparing the oxygen saturation of the mixed venous blood and that of the aorta. When blood shunts left to right at the atrial septal defect it causes the oxygen saturation in the right atrium to rise, however, thorough mixing of blood does not occur in the right atrium but more distally in the right heart circulation, such as in the pulmonary arteries. The higher the oxygen saturation in the pulmonary artery as compared to that of the aorta, the more blood volume shunted left to right at the atrial level.
Incorrect
Correct answer is A:
Atrial septal defect shunt is best measured by comparing the oxygen saturation of the mixed venous blood and that of the aorta. When blood shunts left to right at the atrial septal defect it causes the oxygen saturation in the right atrium to rise, however, thorough mixing of blood does not occur in the right atrium but more distally in the right heart circulation, such as in the pulmonary arteries. The higher the oxygen saturation in the pulmonary artery as compared to that of the aorta, the more blood volume shunted left to right at the atrial level.
Question 22 of 51
22. Question
1 points
Category: Post-operative care in children with heart disease
A 3 year old underwent surgical closure of a large primum atrial septal defect few hours ago. Gradual changes in vital signs were noted over the past few hours associated with prolongation of the capillary refill. Current vital signs are: heart rate 170 bpm, central venous pressure 18 mmHg, blood pressure 75/50 mmHg, oxygen saturation 95%.
Chest x-ray shows a cardiac silhouette larger than earlier in the day.
Echocardiography is likely to show which one of the following?
Correct
Correct !
Elevated central venous pressure and evidence of depressed cardiac output (low blood pressure and narrow pulse pressure as well as prolonged capillary refill) suggest cardiac tamponade secondary to significant pericardial effusion.
Severe aortic regurgitation will cause wide pulse pressure due to drop in diastolic pressure. Pleural effusion will interfere with oxidation and less likely with cardiac output. Dilated cardiac chambers alone cannot explain the elevated central venous pressure and depressed cardiac output.
Incorrect
Correct answer is C:
Elevated central venous pressure and evidence of depressed cardiac output (low blood pressure and narrow pulse pressure as well as prolonged capillary refill) suggest cardiac tamponade secondary to significant pericardial effusion.
Severe aortic regurgitation will cause wide pulse pressure due to drop in diastolic pressure. Pleural effusion will interfere with oxidation and less likely with cardiac output. Dilated cardiac chambers alone cannot explain the elevated central venous pressure and depressed cardiac output.
Question 23 of 51
23. Question
1 points
Category: Post-operative care in children with heart disease
Chylothorax in post-operative care
A 2 year old boy 4 days after completion of Fontan procedure continues to have clear fluid drainage from pleural chest tubes bilaterally. The child continues to be NPO. Microscopic analysis of the fluid shows 78% lymphocyte count.
Which of the following is most appropriate in this child’s management in attempting to reduce pleural effusion?
Correct
Correct !
Despite being clear, the pleural effusion in this child is chyle. The high lymphocyte count is suggestive of the chyle nature of this effusion. he white milky appearance of chyle is due to its high fat contents. This is not present in children who are not feeding orally, rendering the color of effusion clear. Chylothorax is seen in patients with Fontan procedure due to elevation of the central venous pressure which interferes with proper drainage of lymphatic fluid from the gastro-intestinal tract. Reducing the rate of effusion in such patients is done through reduction of volume of chyle through eliminating oral food intake and providing nutrition through total intravenous hyperalimentaion or using diet with medium chain triglycerides.
Incorrect
Correct answer is D:
Despite being clear, the pleural effusion in this child is chyle. The high lymphocyte count is suggestive of the chyle nature of this effusion. The white milky appearance of chyle is due to its high fat contents. This is not present in children who are not feeding orally, rendering the color of effusion clear. Chylothorax is seen in patients with Fontan procedure due to elevation of the central venous pressure which interferes with proper drainage of lymphatic fluid from the gastro-intestinal tract. Reducing the rate of effusion in such patients is done through reduction of volume of chyle through eliminating oral food intake and providing nutrition through total intravenous hyperalimentaion or using diet with medium chain triglycerides.
Question 24 of 51
24. Question
1 points
Category: Post-operative care in children with heart disease
Function of systemic-pulmonary arterial shunt post-operatively
Which of the following parameters is best achieved in a 2 month old with pulmonary atresia, 2 days after surgical placement of a 3.5 mm systemic-pulmonary arterial shunt?
Correct
Correct !
In unprepared cyanotic congenital heart diseases, oxygen saturation depends upon the extent of pulmonary blood flow. �The greater the pulmonary blood flow, the higher the oxygen saturation. �Therefore, almost normal oxygen saturation could be achieved in infants if the pulmonary blood flow is allowed to be very high. �This is detrimental, since the high pulmonary blood flow will result in pulmonary edema and volume overload of the cardiac chambers resulting in congestive heart failure. �Therefore it is always best to aim for an oxygen saturation that does not burden the heart excessively, yet is appropriate for normal growth, such as an oxygen saturation of 75-85%.
The last set of parameters is not ideal since the high heart rate and the low blood pressure may reflect low systemic vascular resistance, which if corrected may lead to elevation of pulmonary blood flow and oxygen saturation.
Incorrect
Correct answer is A:
In unprepared cyanotic congenital heart diseases, oxygen saturation depends upon the extent of pulmonary blood flow. �The greater the pulmonary blood flow, the higher the oxygen saturation. �Therefore, almost normal oxygen saturation could be achieved in infants if the pulmonary blood flow is allowed to be very high. �This is detrimental, since the high pulmonary blood flow will result in pulmonary edema and volume overload of the cardiac chambers resulting in congestive heart failure. �Therefore it is always best to aim for an oxygen saturation that does not burden the heart excessively, yet is appropriate for normal growth, such as an oxygen saturation of 75-85%.
The last set of parameters is not ideal since the high heart rate and the low blood pressure may reflect low systemic vascular resistance, which if corrected may lead to elevation of pulmonary blood flow and oxygen saturation.
Question 25 of 51
25. Question
1 points
Category: Post-operative care in children with heart disease
Understand anatomy of Fontan circuit
In a 2 year old child after Fontan procedure, the venous return from the coronary circulation returns to which one of the following cardiac structures?
Correct
Correct !
The coronary sinus, which drains the myocardium venous circulation, opens into the systemic atrium, thus joining the pulmonary venous blood and causing the oxygen saturation in the single ventricle and out into the systemic circulation to slightly drop. This is why patients with Fontan procedure have somewhat low oxygen saturation (92-95%), even without a Fontan circuit fenestration.
Incorrect
Correct answer is A:
The coronary sinus, which drains the myocardium venous circulation, opens into the systemic atrium, thus joining the pulmonary venous blood and causing the oxygen saturation in the single ventricle and out into the systemic circulation to slightly drop. This is why patients with Fontan procedure have somewhat low oxygen saturation (92-95%), even without a Fontan circuit fenestration.
Question 26 of 51
26. Question
1 points
Category: Post-operative care in children with heart disease
An 8 month old infant underwent complete surgical repair of Tetralogy of Fallot. The child appeared well perfused post-operatively. Heart rate was 120 bpm, regular. Blood pressure is 100/55 by arterial line pressure tracing. Oxygen saturation was 100%. Temperature was 37.2o C. Five hours post-operatively, the peripheral perfusion was reduced; heart rate is 180 bpm, regular. Blood pressure is 60/32. xygen saturation is 100%. Temperature is 39.2o C. The rhythm tracing is shown.
j6
j6
What is the appropriate next step?
Correct
Correct !
The rhythm is that of Junctional ectopic tachycardia (JET), a known complication after surgical repair of Tetralogy of Fallot due to irritation of the atrio-ventricular nodal region. These arrhythmias are malignant since the heart rate is rapid; there is loss of coordination between atrial and ventricular contractions and the compromised myocardium due to surgical repair. Furthermore, these arrhythmias are difficult to treat. In many instances they appear to be precipitated by a rise in the temperature and could be treated or slowed down by lowering the temperature, even to sub normal levels. The only medication which may be helpful is amiodarone intravenously.
Incorrect
Correct answer is C:
The rhythm is that of Junctional ectopic tachycardia (JET), a known complication after surgical repair of Tetralogy of Fallot due to irritation of the atrio-ventricular nodal region. These arrhythmias are malignant since the heart rate is rapid; there is loss of coordination between atrial and ventricular contractions and the compromised myocardium due to surgical repair. Furthermore, these arrhythmias are difficult to treat. In many instances they appear to be precipitated by a rise in the temperature and could be treated or slowed down by lowering the temperature, even to sub normal levels. The only medication which may be helpful is amiodarone intravenously.
Question 27 of 51
27. Question
1 points
Category: Congenital heart disease
ASD 1
A 2 year old girl with an atrial septal defect (ASD) is noted to have a 3/6 systolic ejection murmur at the left upper sternal border and fixed splitting of second heart sound. In addition, there is a 2/4 mid-diastolic murmur at the left lower sternal border. The diastolic murmur indicates that:
Correct
That is Correct!
Murmurs in atrial septal defect are not related to blood flow across the septal defect. The pressure difference between the left and right atria is too small to generate turbulent blood flow, which could be heard as a murmur. Instead, the increase in right heart blood flow will cause turbulent flow across the pulmonary valve leading to the systolic flow murmur. The excessive blood flow across the pulmonic valve will cause it to always close late, resulting in fixed splitting of the second heart sound. If the ASD is large enough it will cause the flow through the right heart to be increased even more causing turbulent flow across the tricuspid valve as well, exhibited in auscultation as a mid-diastolic murmur. Tricuspid blood flow tends to be less turbulent even with increase blood flow through the right heart since it is larger in diameter than the pulmonic valve, but with larger ASD, it will eventually be turbulent enough to cause a heart murmur as well.
Option B is incorrect since pulmonary regurgitation murmur though diastolic, is in early diastole and not mid diastolic. Furthermore, pulmonary regurgitation, due to small pressure differences between the pulmonary artery and the right ventricle during diastole tends to be inaudible.
Option C is incorrect since the size of the ASD does not curtail its closure through cardiac catheterization at this age. Devices are available to close even the very large defects in this age group. It should be noted that at 2 years of age, closure is postponed till about 5 years of age unless there is significant heart failure, not responding to medications.
Option D is incorrect since the type of ASD has no impact on the murmur produced. All types of ASD will produce similar murmurs.
Incorrect
Correct answer is A:
Murmurs in atrial septal defect are not related to blood flow across the septal defect. The pressure difference between the left and right atria is too small to generate turbulent blood flow, which could be heard as a murmur. Instead, the increase in right heart blood flow will cause turbulent flow across the pulmonary valve leading to the systolic flow murmur. The excessive blood flow across the pulmonic valve will cause it to always close late, resulting in fixed splitting of the second heart sound. If the ASD is large enough it will cause the flow through the right heart to be increased even more causing turbulent flow across the tricuspid valve as well, exhibited in auscultation as a mid-diastolic murmur. Tricuspid blood flow tends to be less turbulent even with increase blood flow through the right heart since it is larger in diameter than the pulmonic valve, but with larger ASD, it will eventually be turbulent enough to cause a heart murmur as well.
Option B is incorrect since pulmonary regurgitation murmur though diastolic, is in early diastole and not mid diastolic. Furthermore, pulmonary regurgitation, due to small pressure differences between the pulmonary artery and the right ventricle during diastole tends to be inaudible.
Option C is incorrect since the size of the ASD does not curtail its closure through cardiac catheterization at this age. Devices are available to close even the very large defects in this age group. It should be noted that at 2 years of age, closure is postponed till about 5 years of age unless there is significant heart failure, not responding to medications.
Option D is incorrect since the type of ASD has no impact on the murmur produced. All types of ASD will produce similar murmurs.
Question 28 of 51
28. Question
1 points
Category: Congenital heart disease
ASD 2
A mother of an infant with a 12 mm atrial septal defect (ASD) inquires about the possibility of spontaneous closure of the infant’s ASD. Correct statement regarding ASD spontaneous closure is:
Correct
That is Correct!
Two factors help determine the possibility of spontaneous closure of an ASD. First is type, secundum ASD is the only type amenable to spontaneous closure. Primum and sinus venosus ASD defects are not likely to close spontaneously. The second factor is the size of ASD. Small secundum ASD (smaller than 3 mm) are very likely to close spontaneously, whereas secundum ASD larger than 8 mm are unlikely to close.
Option A is incorrect since medium size ASD (5-8 mm) may close spontaneously, but more than 15% stay open and require intervention for closure.
Option C is incorrect since medium size ASD may still close spontaneously as mentioned above.
Option D is incorrect since secundum ASD, particularly small and medium size are more likely to close than not.
Incorrect
Correct answer is B:
Two factors help determine the possibility of spontaneous closure of an ASD. First is type, secundum ASD is the only type amenable to spontaneous closure. Primum and sinus venosus ASD defects are not likely to close spontaneously. The second factor is the size of ASD. Small secundum ASD (smaller than 3 mm) are very likely to close spontaneously, whereas secundum ASD larger than 8 mm are unlikely to close.
Option A is incorrect since medium size ASD (5-8 mm) may close spontaneously, but more than 15% stay open and require intervention for closure.
Option C is incorrect since medium size ASD may still close spontaneously as mentioned above.
Option D is incorrect since secundum ASD, particularly small and medium size are more likely to close than not.
Question 29 of 51
29. Question
1 points
Category: Congenital heart disease
VSD 1
A 5 year old, known to have a ventricular septal defect (VSD). The VSD is small as shown by previous echocardiograms. Your records indicate that he had a 3/6 holosystolic murmur one year ago. He continues to be asymptomatic with normal physical examination other than the heart murmur, however, auscultation this visit reveals an additional new 2/4 early diastolic murmur at the right upper sternal border. The newly detected murmur indicates that:
Correct
That is Correct!
The newly heard murmur seems to suggest aortic regurgitation, a known complication to perimembrenous and outflow type VSD. This occurs when tan aortic valve cusp becomes involved in the defect causing it to prolapse and eventually become incompetent resulting in regurgitation. This is an indication to close the VSD surgically to reduce risk of further progression of the aortic valve disease.
Option A is incorrect since an increase in pulmonary blood flow due to a VSD will indeed cause a diastolic murmur across the VSD, however, this would be a mid-diastolic murmur at the apex and not an early diastolic murmur at the right upper sternal border. Furthermore, the pulmonary vascular resistance drops in the first few weeks of life and is unlikely to continue to drop at age4-5 years.
Option C is incorrect since it likely that catheter closure at this point is likely to be contraindicated due to the likelihood of involvement of an aortic valve cusp in the VSD. This will prevent proper deployment of the device and further damage to aortic valve.
Option D is incorrect since mitral stenosis produces a mid-diastolic murmur at the apex, not an early diastolic murmur at the right upper sternal border.
Incorrect
Correct answer is B:
The newly heard murmur seems to suggest aortic regurgitation, a known complication to perimembrenous and outflow type VSD. This occurs when tan aortic valve cusp becomes involved in the defect causing it to prolapse and eventually become incompetent resulting in regurgitation. This is an indication to close the VSD surgically to reduce risk of further progression of the aortic valve disease.
Option A is incorrect since an increase in pulmonary blood flow due to a VSD will indeed cause a diastolic murmur across the VSD, however, this would be a mid-diastolic murmur at the apex and not an early diastolic murmur at the right upper sternal border. Furthermore, the pulmonary vascular resistance drops in the first few weeks of life and is unlikely to continue to drop at age4-5 years.
Option C is incorrect since it likely that catheter closure at this point is likely to be contraindicated due to the likelihood of involvement of an aortic valve cusp in the VSD. This will prevent proper deployment of the device and further damage to aortic valve.
Option D is incorrect since mitral stenosis produces a mid-diastolic murmur at the apex, not an early diastolic murmur at the right upper sternal border.
Question 30 of 51
30. Question
1 points
Category: Congenital heart disease
PDA 2
A patent ductus arteriosus (PDA) is surgically closed in which one of the following scenarios?
Correct
Correct !
It is always best to choose the least invasive therapy for any medical condition. In considering the options available for closure of PDA, intravenous indomethacin is the least invasive, though not free of complications as it may cause gastric ulceration, thrmbocytopenia or precipitate renal impairment. Indomethacin works best in premature infants, in the first few days of life. �Therefore the child in option (A) will be best treated with intravenous indomethacin.
Incorrect
Correct answer is C:
It is always best to choose the least invasive therapy for any medical condition. �In considering the options available for closure of PDA, intravenous indomethacin is the least invasive, though not free of complications as it may cause gastric ulceration, thrmbocytopenia or precipitate renal impairment. �Indomethacin works best in premature infants, in the first few days of life. �Therefore the child in option (A) will be best treated with intravenous indomethacin.
Question 31 of 51
31. Question
1 points
Category: Congenital heart disease
AVCD 1
A 6 month old patients with unrepaired complete atrio-ventricular canal defect, including large atrial and ventricular septal defects, has a 3/6 holosystolic murmur heard best over the apical region of the precordium. �This murmur is most commonly attributed to which one of the following hemodynamic factors?
Correct
Correct !
The ventricular septal defect in complete atrioventricular canal defect is typically large, therefore, the left to right shunting across it is laminar and not turbulent, thus does not cause an audible murmur. �On the other hand, atrioventricular valve regurgitation is turbulent and is the cause of murmur in most patients with this congenital heart disease.
Incorrect
Correct answer is B:
The ventricular septal defect in complete atrioventricular canal defect is typically large, therefore, the left to right shunting across it is laminar and not turbulent, thus does not cause an audible murmur. �On the other hand, atrioventricular valve regurgitation is turbulent and is the cause of murmur in most patients with this congenital heart disease.
Question 32 of 51
32. Question
1 points
Category: Congenital heart disease
AS 1
A 12 year old boy is found to have a harsh ejection systolic murmur at the right upper sternal border with radiation to the suprasternal region and an early decrescendo diastolic murmur, heard best over the mid-sternum. The young man is asymptomatic. He is a member of his schools basketball team with no history of easy fatigability, shortness of breath or cyanosis. Hear rate is 65/minute, blood pressure 100/55 mmHg, oxygen saturation is 98%. Physical examination is normal except for the above described heart murmur and a thrill in the suprasternal notch.
Which one of the following heart diseases is most likely to be found in this patient?
Correct
Correct !
The systolic murmur is typical of aortic stenosis, occasionally the systolic murmur is preceded by an ejection click. Murmur is heard best over the right upper sternal border with radiation into the suprasternal notch, where a thrill is palpable. The diastolic murmur most probably reflects aortic regurgitation which may be associated with aortic stenosis due to deformed aortic valve cusps. The murmur of aortic regurgitation is early in diastole and decrescendo in nature.
Murmur of pulmonary stenosis is best heard over the left upper sternal border and those due to patent ductus arteriosus are best heard over the left sub-clavicular region.
Incorrect
Correct answer is A:
The systolic murmur is typical of aortic stenosis, occasionally the systolic murmur is preceded by an ejection click. Murmur is heard best over the right upper sternal border with radiation into the suprasternal notch, where a thrill is palpable. The diastolic murmur most probably reflects aortic regurgitation which may be associated with aortic stenosis due to deformed aortic valve cusps. The murmur of aortic regurgitation is early in diastole and decrescendo in nature.
Murmur of pulmonary stenosis is best heard over the left upper sternal border and those due to patent ductus arteriosus are best heard over the left sub-clavicular region.
Question 33 of 51
33. Question
1 points
Category: Congenital heart disease
AS 2
In a patient with aortic stenosis, which one of the following statements is correct regarding subacute bacterial endocarditis prophylaxis?
Correct
Correct !
All grades of aortic stenosis require prophylaxis, unlike pulmonary valve disease where mild pulmonary stenosis does not require subacute bacterial endocarditis prophylaxis.
Conditions for which endocarditis prophylaxis is recommended
High-risk category
Prosthetic cardiac valves, including bioprosthetic and homograft valves
Previous bacterial endocarditis
Complex cyanotic congenital heart disease (e.g., single ventricle states, transposition of the great arteries, and tetralogy of Fallot)
Surgically constructed systemic-to-pulmonary shunts or conduits
Moderate-risk category
Most other congenital cardiac malformations, such as patent ductus arteriosus, ventricular septal defect, primum atrial septal defect, coarctation of the aorta, and bicuspid aortic valve
Acquired valvar dysfunction (e.g., rheumatic heart disease or collagen vascular disease)
Hypertrophic cardiomyopathy
Mitral valve prolapse with valvar regurgitation and/or thickened leaflets
Conditions for which endocarditis prophylaxis is not recommended
Negligible-risk category (no greater risk than that for the general population)
Isolated secundum atrial septal defect
Surgical repair of atrial septal defect, ventricular septal defect, or patent ductus arteriosus (without residua beyond 6�months)
Previous coronary artery bypass graft surgery
Mitral valve prolapse without valvar regurgitation
Physiologic, functional, or innocent heart murmurs
Previous Kawasaki disease without valvar dysfunction
Previous rheumatic fever without valvar dysfunction
Cardiac pacemakers (intravascular and epicardial) and implanted defibrillators
Incorrect
Correct answer is B:
All grades of aortic stenosis require prophylaxis, unlike pulmonary valve disease where mild pulmonary stenosis does not require subacute bacterial endocarditis prophylaxis.
Conditions for which endocarditis prophylaxis is recommended
High-risk category
Prosthetic cardiac valves, including bioprosthetic and homograft valves
Previous bacterial endocarditis
Complex cyanotic congenital heart disease (e.g., single ventricle states, transposition of the great arteries, and tetralogy of Fallot)
Surgically constructed systemic-to-pulmonary shunts or conduits
Moderate-risk category
Most other congenital cardiac malformations, such as patent ductus arteriosus, ventricular septal defect, primum atrial septal defect, coarctation of the aorta, and bicuspid aortic valve
Acquired valvar dysfunction (e.g., rheumatic heart disease or collagen vascular disease)
Hypertrophic cardiomyopathy
Mitral valve prolapse with valvar regurgitation and/or thickened leaflets
Conditions for which endocarditis prophylaxis is not recommended
Negligible-risk category (no greater risk than that for the general population)
Isolated secundum atrial septal defect
Surgical repair of atrial septal defect, ventricular septal defect, or patent ductus arteriosus (without residua beyond 6�months)
Previous coronary artery bypass graft surgery
Mitral valve prolapse without valvar regurgitation
Physiologic, functional, or innocent heart murmurs
Previous Kawasaki disease without valvar dysfunction
Previous rheumatic fever without valvar dysfunction
Cardiac pacemakers (intravascular and epicardial) and implanted defibrillators
Question 34 of 51
34. Question
1 points
Category: Congenital heart disease
PS 1
Which one of the following changes in auscultation is expected in a child with worsening pulmonary stenosis as compared to previous findings?
Correct
Correct !
In pulmonary stenosis there is systolic click caused by opening of the pulmonary valve. �This is followed by an ejection systolic murmur heard best over the left upper sternal border. �The second component of the second heart sound is caused by closure of the pulmonic valve. �Therefore in pulmonary stenosis, as blood will require more time to go through a stenotic valve, the closure of this valve will be delayed causing widening of splitting of second heart sound, until it completely disappears as the valve becomes too deformed to create a closure sound.
Incorrect
Correct answer is A:
In pulmonary stenosis there is systolic click caused by opening of the pulmonary valve. �This is followed by an ejection systolic murmur heard best over the left upper sternal border. �The second component of the second heart sound is caused by closure of the pulmonic valve. �Therefore in pulmonary stenosis, as blood will require more time to go through a stenotic valve, the closure of this valve will be delayed causing widening of splitting of second heart sound, until it completely disappears as the valve becomes too deformed to create a closure sound.
Question 35 of 51
35. Question
1 points
Category: Congenital heart disease
PS 2
The main pulmonary artery is frequently noted to be dilated in patients with pulmonary stenosis. Which one of the following statement explains the cause for this observation?
Correct
Correct !
The jet produced by forceful blood flow through a narrow pulmonary valve orifice results in dilation of the main pulmonary artery. In addition severe regurgitation of the pulmonary valve, as seen in patients with absent pulmonary valve, may cause dilation of the pulmonary artery.
Incorrect
Correct answer is C:
The jet produced by forceful blood flow through a narrow pulmonary valve orifice results in dilation of the main pulmonary artery. In addition severe regurgitation of the pulmonary valve, as seen in patients with absent pulmonary valve, may cause dilation of the pulmonary artery.
Question 36 of 51
36. Question
1 points
Category: Congenital heart disease
Coarctation of aorta 1
Which one of the following data sets suggests severe coarctation of the aorta in newborn?
k23
k23
Correct
Correct !
The values in set (A) suggest persistent fetal circulation (PFC). Systolic BP in lower extremities is typically slightly higher in lower extremities than that of upper. The lower O2 saturation in the lower extremities suggest right to left shunting at the patent ductus arteriosus.
The values in set (B) are within normal limits.
The values in set (C) suggests severe coarctation of the aorta with low BP in lower extremities and lower saturation due to right to left shunting at the patent ductus arteriosus which is supplying blood flow to the descending aorta in view of coarctation proximal to the ductal insertion into the aorta. The coarctation will be more severe once the ductus arteriosus closes leading to poor cardiac output to the lower extremities, eventually leading to metabolic acidosis and cardiogenic shock.
The values in set (D) suggest cyanotic congenital heart disease with normal aortic arch.
Incorrect
Correct answer is C.
The values in set (A) suggest persistent fetal circulation (PFC). Dystolic BP in lower extremities is typically slightly higher in lower extremities than that of upper. The lower O2 saturation in the lower extremities suggest right to left shunting at the patent ductus arteriosus.
The values in set (B) are within normal limits.
The values in set (C) suggests severe coarctation of the aorta with low BP in lower extremities and lower saturation due to right to left shunting at the patent ductus arteriosus which is supplying blood flow to the descending aorta in view of coarctation proximal to the ductal insertion into the aorta. The coarctation will be more severe once the ductus arteriosus closes leading to poor cardiac output to the lower extremities, eventually leading to metabolic acidosis and cardiogenic shock.
The values in set (D) suggest cyanotic congenital heart disease with normal aortic arch.
Question 37 of 51
37. Question
1 points
Category: Congenital heart disease
Coarctation of aorta 2
Two months after surgical repair of coarctation of the aorta a 12 year old child is doing and is asymptomatic. Blood pressure in the right arm is 155/90 mmHg and right leg 150/88 mmHg. �Heart rate is 80/minute and oxygen saturation is 97% in upper and lower extremities. There is no appreciable murmur on auscultation. What is an appropriate next step in managing this child?
Correct
Correct !
Post-coarcectomy hypertension is a known complication in patients after repair of coarctation of aorta; this is thought to be due to high rennin levels from pre-operative low renal perfusion and/or poor vascular development in post-coarctation region of the body due to low blood flow state for long time. The blood pressure in this patient is significantly elevated in both upper and lower extremities which rules out the possibility of re-coarctation.
Incorrect
Correct answer is C:
Post-coarcectomy hypertension is a known complication in patients after repair of coarctation of aorta; this is thought to be due to high rennin levels from pre-operative low renal perfusion and/or poor vascular development in post-coarctation region of the body due to low blood flow state for long time. The blood pressure in this patient is significantly elevated in both upper and lower extremities which rules out the possibility of re-coarctation.
Question 38 of 51
38. Question
1 points
Category: Congenital heart disease
Tetralogy of Fallot
Tetralogy of Fallot with near normal size of pulmonary arteries undergo repair when the child is 6-12 months of age. Significant delay in repair may result in all of the following complications, EXCEPT one:
Correct
Correct !
Patients with tetralogy of Fallot have decreased pulmonary blood flow due to pulmonary stenosis, which increases in intensity as the child grows. As the extent of pulmonary and right ventricular outflow tract stenosis increase the child becomes more prone to develop Hypercyanotic spells as well as increase incidence of right to left shunting of emboli or septic emboli from the systemic venous circulation to the systemic arterial circulation which may result in stroke or brain abscess. Congestive heart failure may develop if the right ventricle fails, however, this occurs in much older patients and is not associated with increase pulmonary blood flow, which as previously stated is reduced.
Incorrect
Correct answer is B:
Patients with tetralogy of Fallot have decreased pulmonary blood flow due to pulmonary stenosis, which increases in intensity as the child grows. As the extent of pulmonary and right ventricular outflow tract stenosis increase the child becomes more prone to develop Hypercyanotic spells as well as increase incidence of right to left shunting of emboli or septic emboli from the systemic venous circulation to the systemic arterial circulation which may result in stroke or brain abscess. Congestive heart failure may develop if the right ventricle fails, however, this occurs in much older patients and is not associated with increase pulmonary blood flow, which as previously stated is reduced.
Question 39 of 51
39. Question
1 points
Category: Congenital heart disease
Tetralogy of Fallot
An 8 month old, known to have tetralogy of Fallot, is brought to the emergency room due to severe cyanosis following a bout of crying. The child is not responsive and appears intensely cyanotic with poor capillary refill and diminished pulses. Oxygen saturation is not registering when a pulse oximeter is applied. Auscultation reveals a single second heart sound with no systolic or diastolic murmurs. The mother is holding the child in a knee chest position. Which of the following measures is the appropriate next step in managing this child?
Correct
Correct !
This child appears to have a Hypercyanotic spell and is critically ill, therefore, starting an intravenous line may be difficult and require time. Morphine injection subcutaneously may break the cycle and therefore, should be immediately given. In the meantime an intravenous line could be initiated and esmolol or phenylephrine administered. Oxygen will not significantly benefit the child since cyanosis is due lack of pulmonary blood flow.
Incorrect
Correct answer is B:
This child appears to have a Hypercyanotic spell and is critically ill, therefore, starting an intravenous line may be difficult and require time. Morphine injection subcutaneously may break the cycle and therefore, should be immediately given. In the meantime an intravenous line could be initiated and esmolol or phenylephrine administered. Oxygen will not significantly benefit the child since cyanosis is due lack of pulmonary blood flow.
Question 40 of 51
40. Question
1 points
Category: Congenital heart disease
Tricuspid atresia
A 15 month old child with tricuspid atresia underwent recently surgical operation to place a Glen shunt. Which of the following statements is correct?
Correct
Correct !
Glen shunt provides pulmonary blood flow through the superior vena cava which typically is connected to the right pulmonary artery in an end-side fashion. The inferior vena cava continues to drain into the right atrium. The Fontan procedure eventually incorporates venous blood return from the inferior vena cava to the pulmonary circulation. A bi-directional shunt implies that the blood from the superior vena cava flows to both lungs.
Incorrect
Correct answer is D:
Glen shunt provides pulmonary blood flow through the superior vena cava which typically is connected to the right pulmonary artery in an end-side fashion. The inferior vena cava continues to drain into the right atrium. The Fontan procedure eventually incorporates venous blood return from the inferior vena cava to the pulmonary circulation. A bi-directional shunt implies that the blood from the superior vena cava flows to both lungs.
Question 41 of 51
41. Question
1 points
Category: Congenital heart disease
Tricuspid atresia
A 3 month old infant was recently discharged from a hospital after surgical placement of a modified systemic to pulmonary arterial shunt (Blalock-Taussig shunt) for palliation of tricuspid atresia. The child has been feeding orally, though poorly. Weight gain has been slow and the child is currently placed below the 5th percentile for weight. Heart rate is 140/minute, respiratory rate is 40/minute and oxygen saturation is 92%. There is moderate hepatomegaly, no generalized edema. Precordium is hyperactive with prominent apical impulse and no palpable thrill. A 3/6 continuous murmur is heard allover the precordium, but loudest over the right chest.
Which of the following statements is correct regarding the medical condition of this child?
Correct
Correct !
The high oxygen saturation noted in this child indicates significant increase in pulmonary blood flow. Acyanotic congenital heart disease, such as tricuspid atresia will present with increasing oxygen saturation as the pulmonary blood flow increases. High pulmonary blood flow results in improved oxygen saturation since there is larger fully saturated blood volume returning through the pulmonary veins to the heart, thus diluting the poorly saturated oxygen saturation returning from the body. However, this increase in pulmonary blood flow will also cause pulmonary edema and congestive heart failure manifested as tachypnea, tachycardia and failure to thrive. Systemic to pulmonary arterial shunts are fixed in diameter, as the child grows, the shunt size will be relatively smaller with less congestive heart failure. Anti-congestive heart failure medications, such as afterload reducing agents, diuretics and inotropic agents, such as digoxin can bridge the patient until the effective size of the shunt is smaller.
A Glen shunt will be performed eventually, but not at 3 months of age.
Providing oxygen supplementation will only reduce pulmonary vascular resistance more and result in further increase of pulmonary blood flow and congestive heart failure.
Incorrect
Correct answer is B:
The high oxygen saturation noted in this child indicates significant increase in pulmonary blood flow. Acyanotic congenital heart disease, such as tricuspid atresia will present with increasing oxygen saturation as the pulmonary blood flow increases. High pulmonary blood flow results in improved oxygen saturation since there is larger fully saturated blood volume returning through the pulmonary veins to the heart, thus diluting the poorly saturated oxygen saturation returning from the body. However, this increase in pulmonary blood flow will also cause pulmonary edema and congestive heart failure manifested as tachypnea, tachycardia and failure to thrive. Systemic to pulmonary arterial shunts are fixed in diameter, as the child grows, the shunt size will be relatively smaller with less congestive heart failure. Anti-congestive heart failure medications, such as afterload reducing agents, diuretics and inotropic agents, such as digoxin can bridge the patient until the effective size of the shunt is smaller.
A Glen shunt will be performed eventually, but not at 3 months of age.
Providing oxygen supplementation will only reduce pulmonary vascular resistance more and result in further increase of pulmonary blood flow and congestive heart failure.
Question 42 of 51
42. Question
1 points
Category: Congenital heart disease
A newborn presents with extreme cyanosis at birth. Oxygen saturation is 30% despite 100% supplemental oxygen. The baby is born at full term, uncomplicated gestation. Birth weight is 2.8 kg. There is no history of meconium aspiration. Except for profound cyanosis, the physical examination is within normal limits. Which one of the following cyanotic congenital heart diseases is most likely in this child?
Correct
Correct !
Patients with transposition of the great vessels, especially those without a ventricular septal defect are extremely cyanotic at birth.
Incorrect
Correct answer is A:
Patients with transposition of the great vessels, especially those without a ventricular septal defect are extremely cyanotic at birth.
Question 43 of 51
43. Question
1 points
Category: Congenital heart disease
Transposition of the great arteries
A 5 day old boy was diagnosed to have transposition of the great arteries on the first day of life. Echo guided Rashkind atrial septostomy was performed soon after birth resulting in significant improvement in oxygen saturation. The baby has been stable since then with oxygen saturation between 75% and 85%. Physical examination shows a full term baby with mild cyanosis and good capillary refill. Precordium is mildly hyperactive with no palpable thrill. First heart sound is normal, second heart sound is single throughout the respiratory cycle. Why is the second heart sound single?
Correct
Correct !
In transposition of the great arteries, the pulmonary valve becomes posterior, which places it further away from the sternum and consequently the stethoscope. �On the other hand the aortic valve is anterior and closer to the sternum. The loud nearby aortic valve and the soft further away pulmonary valve result in a single heart sound. On the other hand, it really is difficult to appreciate the splitting of second heart sound even in normal newborns in view of their rapid heart rate. Therefore, the issue of single heart sound in babies with transposition of the great arteries becomes a matter of roundmanship� rather than any real benefit in clinical assessment.
Incorrect
Correct answer is D:
In transposition of the great arteries, the pulmonary valve becomes posterior, which places it further away from the sternum and consequently the stethoscope. On the other hand the aortic valve is anterior and closer to the sternum. The loud nearby aortic valve and the soft further away pulmonary valve result in a single heart sound. On the other hand, it really is difficult to appreciate the splitting of second heart sound even in normal newborns in view of their rapid heart rate. Therefore, the issue of single heart sound in babies with transposition of the great arteries becomes a matter of roundmanship rather than any real benefit in clinical assessment.
Question 44 of 51
44. Question
1 points
Category: Congenital heart disease
Truncus arteriosus
A one week old baby, known to have truncus arteriosus develops seizures. Work up includes serum electrolytes which demonstrate low serum calcium. Hypocalcemia persists despite multiple intravenous calcium infusions. What other organ failure should be suspected in this child.
Correct
Correct !
This child is likely to have DiGeorge syndrome which includes defects of the heart (outflow abnormalities), parathyroid gland and thymus gland. Failure of proper development of the thymus will cause T-cells immune deficiency. Not all patients with positive DiGeorge gene test are complete in their presentation, i.e. not all defect may be manifested.
Incorrect
Correce Answer: C
This child is likely to have DiGeorge syndrome which includes defects of the heart (outflow abnormalities), parathyroid gland and thymus gland. Failure of proper development of the thymus will cause T-cells immune deficiency. Not all patients with positive DiGeorge gene test are complete in their presentation, i.e. not all defect may be manifested.
Question 45 of 51
45. Question
1 points
Category: Congenital heart disease
Total anomalous pulmonary venous return
A few hour old newborn is noted to have cyanosis. Oxygen saturation is 75% while breathing room air. Physical examination is significant for cyanosis and mild respiratory distress, but is otherwise within normal limits. Chest x-ray is described to have snowman appearance. Which one of the following differential diagnosis is most likely in this child?
k23
k23
Correct
Correct !
The snowman appearance refers to the 2 circular shadows, one on top of the other simulating figure 8 or a snowman. This is produced by the cardiac shadow making the lower round structure and the anomalous veins as the collect into a single vertical vein which ascends to meet a dilated innominant vein which runs horizontally to the right to meet the superior vena cava.
All other choices are associated with a narrow mediastinum due to abnormal antero-posterior relationship as in transposition of the great vessels and corrected transposition, or a single great vessel as in truncus arteriosus.
Incorrect
Correct answer is C:
The snowman appearance refers to the 2 circular shadows, one on top of the other simulating figure 8 or a snowman. This is produced by the cardiac shadow making the lower round structure and the anomalous veins as the collect into a single vertical vein which ascends to meet a dilated innominant vein which runs horizontally to the right to meet the superior vena cava.
All other choices are associated with a narrow mediastinum due to abnormal antero-posterior relationship as in transposition of the great vessels and corrected transposition, or a single great vessel as in truncus arteriosus.
Question 46 of 51
46. Question
1 points
Category: Congenital heart disease
Total anomalous pulmonary venous return
In total anomalous pulmonary venous return, all pulmonary veins drain in an anomalous fashion to structures other than the left atrium. The anomalous drainage could be to a variety of locations. Which of the following cardiac structures is not a known site for the anomalous pulmonary veins to drain to?
Correct
Correct !
Pulmonary veins drain into any of the systemic venous structures close to the heart such as superior and inferior vena cavae, right atrium and coronary sinus. These structures have lower pressures than that of the pulmonary veins, thus facilitating blood flow. On the other hand, the right ventricle has a higher pressure than the pulmonary veins which would prevent such a connection. Furthermore, the right ventricle is embryologically very distinct from the pulmonary veins, while the other structures listed above are in close proximity, which could lead to this embryological mal-development.
Incorrect
Correct answer is D:
Pulmonary veins drain into any of the systemic venous structures close to the heart such as superior and inferior vena cavae, right atrium and coronary sinus. These structures have lower pressures than that of the pulmonary veins, thus facilitating blood flow. On the other hand, the right ventricle has a higher pressure than the pulmonary veins which would prevent such a connection. Furthermore, the right ventricle is embryologically very distinct from the pulmonary veins, while the other structures listed above are in close proximity, which could lead to this embryological mal-development.
Question 47 of 51
47. Question
1 points
Category: Congenital heart disease
Anomalous coronary artery from pulmonary artery
A 6 month old girl presents to the emergency room with shortness of breath, pallor and poor feeding. Chest x-ray reveals a severely enlarged heart and significant pulmonary edema. �An earlier chest x-ray performed for unrelated reasons show normal heart size and lung fields at 2 weeks of age. Echocardiography shows anomalous left coronary artery from pulmonary artery.
Which one of the following statements accurately describes the reason for a normal chest x-ray at 2 weeks of life versus the abnormal findings at 6 months of life?
Correct
Correct !
When the left coronary artery originates in an anomalous fashion from the pulmonary artery, it is capable of supplying blood to the myocardium due to the high pulmonary vascular resistance and consequently high pressures while in-utero and soon after birth. However, as the pulmonary vascular resistance drops, the driving force to perfuse the anomalous left coronary artery drops, resulting in poor perfusion of the myocardium, causing myocardial infarction. Therefore, it is not unusual to have normal appearing heart in the first few weeks of life, but as pulmonary vascular resistance drops, the perfusion in the left coronary artery also drops, resulting in myocardial infarction and dilated cardiomyopathy.
Incorrect
Correct answer is C:
When the left coronary artery originates in an anomalous fashion from the pulmonary artery, it is capable of supplying blood to the myocardium due to the high pulmonary vascular resistance and consequently high pressures while in-utero and soon after birth. However, as the pulmonary vascular resistance drops, the driving force to perfuse the anomalous left coronary artery drops, resulting in poor perfusion of the myocardium, causing myocardial infarction. Therefore, it is not unusual to have normal appearing heart in the first few weeks of life, but as pulmonary vascular resistance drops, the perfusion in the left coronary artery also drops, resulting in myocardial infarction and dilated cardiomyopathy.
Question 48 of 51
48. Question
1 points
Category: Congenital heart disease
Anomalous coronary artery from pulmonary artery
Patients with anomalous left coronary artery from pulmonary artery develop infarction of the myocardium. �This is caused by which one of the following factors?
Correct
Correct !
The oxygen saturation in the pulmonary arteries is about 75%, which is adequate to perfuse tissue. However, it is the low driving force due to dropping of pulmonary vascular resistance after birth that result in myocardial infarction. Coronary arterial branching is normal in this lesion and not known to be associated with coronary arterial stenosis.
Incorrect
Correct answer is A:
The oxygen saturation in the pulmonary arteries is about 75%, which is adequate to perfuse tissue. However, it is the low driving force due to dropping of pulmonary vascular resistance after birth that result in myocardial infarction. Coronary arterial branching is normal in this lesion and not known to be associated with coronary arterial stenosis.
Question 49 of 51
49. Question
1 points
Category: Congenital heart disease
Vascular ring
A 6 month old boy with chronic stridor and repeated admissions for respiratory distress was noted to have indentation of the tracheal shadow by chest x-ray. The indentation was on both sides of the trachea (right and left sides). Barium swallow performed show esophageal indentation, again on both sides of the esophagus.
Which one of the following diagnosis is most likely?
Correct
Correct !
Each of the first 3 choices causes a vascular ring, resulting in compression of the trachea with or without compression of the esophagus as well. These patients present with respiratory distress and may also have dysphagia.
In this particular case there is compression of the trachea and esophagus bilaterally, indicating that the compression structures surround the esophagus and trachea from the left and right sides, this is seen in double aortic arch. Whereas in right aortic arch with aberrant left subclavian artery and pulmonary sling, the trachea is compressed from the right and posterior aspects and the esophagus is compressed anteriorly.
The fourth choice does not cause vascular ring.
Incorrect
Correct answer is B:
Each of the first 3 choices causes a vascular ring, resulting in compression of the trachea with or without compression of the esophagus as well. These patients present with respiratory distress and may also have dysphagia.
In this particular case there is compression of the trachea and esophagus bilaterally, indicating that the compression structures surround the esophagus and trachea from the left and right sides, this is seen in double aortic arch. Whereas in right aortic arch with aberrant left subclavian artery and pulmonary sling, the trachea is compressed from the right and posterior aspects and the esophagus is compressed anteriorly.
The fourth choice does not cause vascular ring.
Question 50 of 51
50. Question
1 points
Category: Congenital heart disease
Vascular ring
An 8 month old infant was diagnosed to have a vascular ring caused by a right aortic arch and aberrant left subclavian artery. The vascular structures completed a ring around the esophagus since the right aortic arch was to the left of the trachea, then traverses in an abnormal fashion the space between the esophagus and trachea, the aberrant left subclavian artery takes off from the descending aorta just left of the trachea and is connected through a small patent ductus arteriosus which runs to the left of the trachea and connects to the main pulmonary-left pulmonary artery junction, thus completing the ring around the trachea. The decision was made in the cardiac catheterization laboratory after detecting these findings to refer the child for surgical ligation and division of the patent ductus arteriosus to relief the vascular ring.
Why was this procedure not attempted in the cardiac catheterization laboratory through coil occlusion of the ductus arteriosus?
Correct
Correct !
The vascular ring formed by a right aortic arch and aberrant left subclavian artery is completed by the ductus arteriosus connecting the aberrant left subclavian artery to the pulmonary artery. A vascular ring will still be present even if there is no flow across the patent ductus arteriosus (i.e. a ductal ligament), since the ductal ligament still completes the vascular ring around the trachea. Therefore, the ductal ligament or ductus arteriosus must be divided to offer a relief of the vascular ring. Re-implantation of the aberrant left subclavian artery is not necessary to disrupt the vascular ring.
Incorrect
Correct answer is A:
The vascular ring formed by a right aortic arch and aberrant left subclavian artery is completed by the ductus arteriosus connecting the aberrant left subclavian artery to the pulmonary artery. A vascular ring will still be present even if there is no flow across the patent ductus arteriosus (i.e. a ductal ligament), since the ductal ligament still completes the vascular ring around the trachea. Therefore, the ductal ligament or ductus arteriosus must be divided to offer a relief of the vascular ring. Re-implantation of the aberrant left subclavian artery is not necessary to disrupt the vascular ring.
Question 51 of 51
51. Question
1 points
Category: Congenital heart disease
Anomalous origin of left coronary artery
A 16 year old young man participates in competitive sports. He collapsed during a basketball game. He was asymptomatic prior to this incident and after brief loss of consciousness appeared perfectly normal. Physical examination, chest x-ray, electrocardiogram and serum cardiac enzymes were all within normal limits in the emergency room. Echocardiography showed normal cardiac structure and function with a left coronary artery origin from the right coronary cusp, the left coronary artery then coursed between the aorta and pulmonary artery, then bifurcated, in a normal fashion into the left anterior descending and circumflex arteries.
What should the next step be in managing this young man?
Correct
Correct !
Origin of the left coronary artery from the right coronary artery sinus will cause it to course in between the two great vessels which is likely to compress it in conditions of increased cardiac output, such as with exercise. This anomaly must be corrected as life threatening compromise to blood flow through the left coronary artery is likely to occur with exercise, particularly in an athlete. Treadmill stress test is dangerous to perform and will not alter recommendations weather positive or negative in its findings. Arrhythmia monitoring is not very helpful in decision making.
Incorrect
Correct answer is C:
Origin of the left coronary artery from the right coronary artery sinus will cause it to course in between the two great vessels which is likely to compress it in conditions of increased cardiac output, such as with exercise. This anomaly must be corrected as life threatening compromise to blood flow through the left coronary artery is likely to occur with exercise, particularly in an athlete. Treadmill stress test is dangerous to perform and will not alter recommendations weather positive or negative in its findings. Arrhythmia monitoring is not very helpful in decision making.
Time limit: 0
Quiz-summary
0 of 21 questions completed
Questions:
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
Information
CCHD Exam – Part IV
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You must sign in or sign up to start the quiz.
You have to finish following quiz, to start this quiz:
Results
0 of 21 questions answered correctly
Your time:
Time has elapsed
You have reached 0 of 0 points, (0)
Average score
Your score
Categories
Acquired heart disease in children0%
Pediatric cardiology pharmacology0%
Congratulations on a job well done!
Your result has been entered into leaderboard
Loading
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
Answered
Review
Question 1 of 21
1. Question
1 points
Category: Acquired heart disease in children
Dilated cardiomyopathy
A 2 year old boy presents with shortness of breath, tachypnea and easy fatigability. Past medical history is significant for recent history of viral upper respiratory infection. Family history is non-contributory. Heart rate is 120 beats per minute, respiratory rate is 40 per minute. Blood pressure is 60/30 mmHg in the right upper extremity. Peripheral pulses are weak. Abdomen is soft and the liver edge is at 6 cm below right costal margin. Precordium is active with increase right and left ventricular impulses. A holosystolic murmur, 3/6 in intensity is heard at the apical region.
Chest x-ray shows cardiomegaly (0.7 cardio-thoracic ratio) with prominent vascular markings in the lung fields.
Echocardiography shows normal cardiac structure. The left ventricle is severely dilated with poor function and moderate mitral regurgitation.
White blood count is mildly elevated with 80% lymphocytes. Erythrocyte sedimentation rate and C-reactive protein are both elevated.
Presumptive diagnosis is dilated cardiomyopathy secondary to myocarditis.
Which one of the following statements is correct regarding this case?
Correct
That is Correct!
Infectious myocarditis is caused by viral infection, bacteria, protozoa and rickettsia, though viral myocarditis tends to be more prevalent. Enteroviruses, such as coxsackie are common causes of viral myocarditis. Non-infectious myocarditis, such as Kawasaki or Takayasu’s disease may also cause dilated cardiomyopathy. Hypertrophic cardiomyopathy is not known to be caused by viral infections.
Incorrect
Correct answer is C:
Infectious myocarditis is caused by viral infection, bacteria, protozoa and rickettsia, though viral myocarditis tends to be more prevalent. Enteroviruses, such as coxsackie are common causes of viral myocarditis. Non-infectious myocarditis, such as Kawasaki or Takayasu’s disease may also cause dilated cardiomyopathy. Hypertrophic cardiomyopathy is not known to be caused by viral infections.
Question 2 of 21
2. Question
1 points
Category: Pediatric cardiology pharmacology
Digoxin
A 2 year child was started on intravenous digoxin, this included intravenous loading and 2 days of maintenance intravenous digoxin administration, a therapeutic level was successfully achieved. What is the appropriate total daily dose of digoxin which should be used when switching to oral digoxin?
Correct
That is Correct!
Bioavailability of oral digoxin is 75% of that of the intravenous format, therefore, higher doses should be given orally (about 130%). The usual daily dose of digxin to children outside the neonatal period is 10 microgram per kilogram per day.
Incorrect
Correct answer is C:
Bioavailability of oral digoxin is 75% of that of the intravenous format, therefore, higher doses should be given orally (about 130%). The usual daily dose of digxin to children outside the neonatal period is 10 microgram per kilogram per day.
Question 3 of 21
3. Question
1 points
Category: Acquired heart disease in children
Dilated cardiomyopathy
Dilated cardiomyopathy is associated with all the following, except one. Identify the lesion/condition which is not associated with dilated cardiomyopathy.
Correct
That is Correct!
Prolonged use of steroids may result in hypertrophic, not dilated cardiomyopathy. Prolonged steroid therapy in young infants and premature neonates induces increased protein synthesis in myocytes, leading to hypertrophy of ventricular walls, typically manifesting as concentric left and right ventricular hypertrophy. Friedreich’s ataxia, Duchenne muscular dystrophy and Becker’s dystrophy are all associated with dilated cardiomyopathy. Duchenne muscular dystrophy is an autosomal dominant trait, while Becker muscular dystrophy is an X-linked trait. The genetic mutation in these conditions causes no (Duchenne) or deformed (Becker) production of dytrophin, an important protein in the function of skeletal and myocardial cells. This results in skeletal and myocardial muscle disease in Duchenne muscular dystrophy and mild skeletal but significant myocardial muscle disease in Becker’s muscular dystrophy.
Incorrect
Correct answer is A:
Prolonged use of steroids may result in hypertrophic, not dilated cardiomyopathy. Prolonged steroid therapy in young infants and premature neonates induces increased protein synthesis in myocytes, leading to hypertrophy of ventricular walls, typically manifesting as concentric left and right ventricular hypertrophy. Friedreich’s ataxia, Duchenne muscular dystrophy and Becker’s dystrophy are all associated with dilated cardiomyopathy. Duchenne muscular dystrophy is an autosomal dominant trait, while Becker muscular dystrophy is an X-linked trait. The genetic mutation in these conditions causes no (Duchenne) or deformed (Becker) production of dytrophin, an important protein in the function of skeletal and myocardial cells. This results in skeletal and myocardial muscle disease in Duchenne muscular dystrophy and mild skeletal but significant myocardial muscle disease in Becker’s muscular dystrophy.
Question 4 of 21
4. Question
1 points
Category: Acquired heart disease in children
Hypertrophic cardiomyopathy
A newborn with 8 and 9 Apgar scores at 1 and 5 minutes. At 2 days of life a 3/6 systolic ejection murmur at right upper sternal border and mid sternum was detected. Physical examination is otherwise within normal limits.
Echocardiographic evaluation revealed hypertrophic cardiomyopathy with mild to moderate left ventricular outflow obstruction (45 mmHg pressure gradient).
Which of the following causes for hypertrophic cardiomyopathy predicts a possible good outcome?
Correct
That is Correct!
Hypertrophic cardiomyopathy typically progresses as child gets older. Presentation in the neonatal period is a sign of poor outcome, except in cases of maternal diabetes. The high glucose level in maternal and fetal circulation causes high level of fetal insulin production. This leads to macrosomia and hypertrophy of the ventricular walls, leading to left ventricular outflow obstruction. Such neonates may be born ill, however, improvement is expected in most cases as the environment of high glucose and insulin resolves after delivery.
Incorrect
Correct answer is B:
Hypertrophic cardiomyopathy typically progresses as child gets older. Presentation in the neonatal period is a sign of poor outcome, except in cases of maternal diabetes. The high glucose level in maternal and fetal circulation causes high level of fetal insulin production. This leads to macrosomia and hypertrophy of the ventricular walls, leading to left ventricular outflow obstruction. Such neonates may be born ill, however, improvement is expected in most cases as the environment of high glucose and insulin resolves after delivery.
Question 5 of 21
5. Question
1 points
Category: Acquired heart disease in children
Hypertrophic cardiomyopathy
A 16 year old girl is known to have hypertrophic cardiomyopathy; previous echocardiograms demonstrate asymmetrical septal hypertrophy with a pressure gradient of 50 mmHg across the left ventricular outflow tract. This is thought to be of the familial type. Patient complains of occasional dyspnea and palpitation. Past medical history is significant for syncope. Previous Holter monitor studies indicate premature ventricular ectopy. All of the following medications are helpful in managing this patient, except one. Which of the following medications is contraindicated in this patient?
Correct
That is Correct!
Beta blockers such as atenolol are helpful in reducing dyspnea in patient with hypertrophic cardiomyopathy. It is a negative inotropic agent which reduces left ventricular outflow obstruction and an anti-arrhythmic agent which prevents ventricular arrhythmias. Amiodarone and Verapamil also reduce ventricular arrhythmia and are known to reduce the risk of sudden death. On the other hand enalpril is an after-load reducing agent which may cause exaggeration of left ventricular outflow tract obstruction, and as such its use is contra-indicated.
Incorrect
Correct answer is D:
Beta blockers such as atenolol are helpful in reducing dyspnea in patient with hypertrophic cardiomyopathy. It is a negative inotropic agent which reduces left ventricular outflow obstruction and an anti-arrhythmic agent which prevents ventricular arrhythmias. Amiodarone and Verapamil also reduce ventricular arrhythmia and are known to reduce the risk of sudden death. On the other hand enalpril is an after-load reducing agent which may cause exaggeration of left ventricular outflow tract obstruction, and as such its use is contra-indicated.
Question 6 of 21
6. Question
1 points
Category: Acquired heart disease in children
Rheumatic heart disease
A 7 year old girl presents with a 3 day history of fever, rash and joint pain affecting ankles and knee joints bilaterally. Heart rate is 100 beats per minute, respiratory rate is 25 per minute. Oral temperature is 38 o Celsius. Blood pressure is 110/60 in right upper extremity; oxygen saturation is 95% while breathing room air. Maculopapular rash covers the extremities and trunk. Good peripheral pulses and perfusion. Abdomen is soft, no hepatomegaly or spleenomegaly detected. A soft 2/6 systolic ejection murmur is heard over the left upper sternal border with no appreciable radiation. Murmur disappears with Valsalva maneuver. No evidence of joint inflammation is present.
Chest x-ray is normal. White blood count is mildly elevated; erythrocyte sedimentation rate is 25 with positive C-reactive protein.
Which of the following statements is correct regarding rheumatic fever’s Jones criteria in this case?
Correct
That is Correct!
This case provides none of the major criteria of Jones (carditis, polyarthritis, chorea, eryhtema marginatum and sub-coetaneous nodules). Therefore, diagnosis of rheumatic fever is not possible in this case. The murmur detected is not consistent with any of the known cardiac lesions in rheumatic fever (aortic regurgitation or mitral regurgitation). The murmur appears to be an innocent heart murmur as it is soft, systolic and disappear with Valsalva maneuver. The joint pain is arthralgia, minor criteria as physical examination reveals no evidence of arthritis. The rash is non-specific and does not have the appearance of eryhtema marginatum (raised edges).
Incorrect
Correct answer is D:
This case provides none of the major criteria of Jones (carditis, polyarthritis, chorea, eryhtema marginatum and sub-coetaneous nodules). Therefore, diagnosis of rheumatic fever is not possible in this case. The murmur detected is not consistent with any of the known cardiac lesions in rheumatic fever (aortic regurgitation or mitral regurgitation). The murmur appears to be an innocent heart murmur as it is soft, systolic and disappear with Valsalva maneuver. The joint pain is arthralgia, minor criteria as physical examination reveals no evidence of arthritis. The rash is non-specific and does not have the appearance of eryhtema marginatum (raised edges).
Question 7 of 21
7. Question
1 points
Category: Acquired heart disease in children
Rheumatic heart disease
A 10 year old boy presents with a 3 day history of fever, rash and joint pain affecting ankles and knee joints bilaterally. Heart rate is 100 beats per minute, respiratory rate is 25 per minute. Oral temperature is 38 o Celsius. Blood pressure is 110/60 in right upper extremity; oxygen saturation is 95% while breathing room air. A rash with raised edges covers the extremities and trunk. Good peripheral pulses and perfusion. Abdomen is soft, no hepatomegaly or spleenomegaly detected. A soft 3/6 holosystolic murmur is heard over the cardiac apex.
Chest x-ray is normal. White blood count is mildly elevated; erythrocyte sedimentation rate is 25 with positive C-reactive protein.
Which of the following statements is correct regarding management of this case?
Correct
That is Correct!
This case is consistent with rheumatic fever. Prednisone is recommended in cases of pancarditis to hasten control of inflammation which may worsen cardiac involvement. A short course of steroids over 2 weeks should be followed with a longer course of acetyl salicylic acid to maintain anti-inflammatory effect. Acetyl salicylic acid is typically used for 2-3 months, guided by inflammatory markers such as fever, erythrocyte sedimentation rate and C-reactive protein.
Incorrect
Correct answer is B:
This case is consistent with rheumatic fever. Prednisone is recommended in cases of pancarditis to hasten control of inflammation which may worsen cardiac involvement. A short course of steroids over 2 weeks should be followed with a longer course of acetyl salicylic acid to maintain anti-inflammatory effect. Acetyl salicylic acid is typically used for 2-3 months, guided by inflammatory markers such as fever, erythrocyte sedimentation rate and C-reactive protein.
Question 8 of 21
8. Question
1 points
Category: Acquired heart disease in children
Kawasaki
A 6 month old boy presents with diffuse maculopapular rash, high fever and anorexia for 3 days. Patient appears irritable with no respiratory distress. Heart rate is 140 beats per minute, respiratory rate is 35 per minute, blood pressure in right upper extremity is 100/60 mmHg, oral temperature is 39o Celsius. Bilateral, non-purulent conjunctivitis is noted. Cervical lymph nodes are enlarged. Peripheral pulses and perfusion are good. Abdomen is soft, no hepatomegaly is detected. Cardiac and pulmonary examination is within normal limits.
Which of the following statements is NOT correct regarding management of this case?
Correct
That is Correct!
Management of Kawasaki disease involves anti-inflammatory and anti-platelet agents. Anti-inflammatory agents reduce the inflammatory process to minimize consequences, particularly those pertaining to coronary arterial disease. Once signs of inflammation subside, aspirin dose could be reduced to anti-platelet low levels. To achieve the latter either approaches as in statements “A” or “B” can be used. Cardiology follow up should be maintained long term, even with no evidence of cardiac involvement since there is evidence that patients may develop early coronary arterial disease even in the absence of initial coronary arterial aneurysm.
Incorrect
Correct answer is D:
Management of Kawasaki disease involves anti-inflammatory and anti-platelet agents. Anti-inflammatory agents reduce the inflammatory process to minimize consequences, particularly those pertaining to coronary arterial disease. Once signs of inflammation subside, aspirin dose could be reduced to anti-platelet low levels. To achieve the latter either approaches as in statements “A” or “B” can be used. Cardiology follow up should be maintained long term, even with no evidence of cardiac involvement since there is evidence that patients may develop early coronary arterial disease even in the absence of initial coronary arterial aneurysm.
Question 9 of 21
9. Question
1 points
Category: Acquired heart disease in children
Kawasaki
Patients with Kawasaki disease are known to develop coronary arterial aneurysm. Which one of the following complications is also known to occur in these patients?
Correct
That is Correct!
Cardiac involvement in Kawasaki disease includes coronary arterial aneurysm and later stenosis, myocarditis, vlavulitis and valvular regurgitation of aortic and mitral valves. Mitral regurgitation may be a result of vlavulitis and /or papillary muscle ischemia due to myocarditis and/or coronary arterial occlusion.
Incorrect
Correct answer is B:
Cardiac involvement in Kawasaki disease includes coronary arterial aneurysm and later stenosis, myocarditis, vlavulitis and valvular regurgitation of aortic and mitral valves. Mitral regurgitation may be a result of vlavulitis and /or papillary muscle ischemia due to myocarditis and/or coronary arterial occlusion.
Question 10 of 21
10. Question
1 points
Category: Acquired heart disease in children
Sub-acute bacterial endocarditis
A 5 year old boy is undergoing chemotherapy course for leukemia. Few months ago a central venous line was placed; the tip of the catheter appears to be at the superior vena cava-right atrium junction by chest x-ray. The child now presents with fever of 103o F. He is lethargic with no respiratory distress. White blood cell count is 23,000/mm3 with 60% leukocytes and 15% bands. Blood cultures were obtained, results pending. An echocardiogram performed to assess ventricular function and central venous line shows brisk left ventricular function, the tip of the central venous line is seen at the distal superior vena cava with no evidence of clots or vegetations.
Which of the following statements is correct statement regarding management of this child?
Correct
That is Correct!
Subacute bacterial endocarditis is a known complication of central venous lines within the heart or central veins. This may manifest as a vegetation seen at the tip of the catheter, however, this is not necessary to be present as the infectious process may be microscopic and not visualized be echocardiography. Subacute bacterial endocarditis is diagnosed by a constellation of symptoms and signs indicating generalized and severe infection as well as positive blood culture. Diagnosis is initially presumptive and treatment with wide spectrum antibiotics is initiated until diagnosis is established. Multiple antibacterial agents are typically used for prolonged period of times. Central venous lines need not be removed if peripheral blood culture is positive while blood cultures from the central line is negative since the central line may not be involved in the infection.
Incorrect
Correct answer is A:
Subacute bacterial endocarditis is a known complication of central venous lines within the heart or central veins. This may manifest as a vegetation seen at the tip of the catheter, however, this is not necessary to be present as the infectious process may be microscopic and not visualized be echocardiography. Subacute bacterial endocarditis is diagnosed by a constellation of symptoms and signs indicating generalized and severe infection as well as positive blood culture. Diagnosis is initially presumptive and treatment with wide spectrum antibiotics is initiated until diagnosis is established. Multiple antibacterial agents are typically used for prolonged period of times. Central venous lines need not be removed if peripheral blood culture is positive while blood cultures from the central line is negative since the central line may not be involved in the infection.
Question 11 of 21
11. Question
1 points
Category: Acquired heart disease in children
Sub-acute bacterial endocarditis
A 3 year old with secundum atrial septal defect will be undergoing a dental procedure. Child is active with no easy fatigability, shortness of breath or cyanosis. HR 100 beats per minute, respiratory rate 25 per minute, oxygen saturation is 99%. Physical examination is within normal limits, except for a 2/6 ejection systolic murmur at the left upper sternal border.
Which of the following recommendations is correct regarding subacute bacterial endocarditis management?
Correct
That is Correct!
Secundum atrial septal defect does not require prophylaxis for subacute bacterial endocarditis.
Conditions for which endocarditis prophylaxis is recommended
High-risk category
•Prosthetic cardiac valves, including bioprosthetic and homograft valves
•Previous bacterial endocarditis
•Complex cyanotic congenital heart disease (e.g. single ventricle states, transposition of the great arteries, tetralogy of Fallot)
•Surgically constructed systemic to pulmonary shunts or conduits
Moderate-risk category
•Most other congenital cardiac malformations such as: patent ductus arteriosus, ventricular septal defect, primum atrial septal defect, coarctation of the aorta and bicuspid aortic valve.
•Mitral valve prolapse with valvar regurgitation and/or thickened leaflets
Conditions for which endocarditis prophylaxis is not recommended
Negligible-risk category (no greater risk than the general population)
•Isolated secundum atrial septal defect
•Surgical repair of atrial septal defect, ventricular septal defect, or patent ductus arteriosus (without residua beyond 6 months)
•Previous coronary artery bypass graft surgery
•Mitral valve prolapse without valvar regurgitation1
•Physiologic, functional, or innocent heart murmurs1
•Previous Kawasaki disease without valvar dysfunction
•Previous rheumatic fever without valvar dysfunction
•Cardiac pacemakers (intravascular and epicardial) and implanted defibrillators
Prophylactic Regimens for Dental, Oral, Respiratory Tract, or Esophageal Procedures (Follow-up dose no longer recommended.) Total children’s dose should not exceed adult dose.
A.Standard general prophylaxis for patients at risk:
Amoxicillin: Adults, 2.0g (children, 50 mg/kg) given orally one hour before procedure.
B.Unable to take oral medications:
Ampicillin: Adults 2.0 g (children, 50 mg/kg) given IM or IV within 30 minutes before procedure.
Clindamycin: Adults, 600 mg (children 20 mg/kg) orally one hour before procedure.
-OR-
Cephalexin or Cefadroxil: Adults 2.0 g (children 50 mg/kg) orally one hour before procedure. (Cephalosporins should not be used in patients with immediate-type hypersensitivity reaction to penicillin).
-OR-
Azithromycin or Clarithromycin: Adults, 500mg (children, 15 mg/kg) orally one hour before procedure.
D.Amoxicillin/ampicillin/penicillin-allergic patients unable to take oral medications:
Clindamycin: Adults, 600 mg (children, 20 mg/kg) IV within 30 minutes before procedure.
-OR-
Cefazolin: Adults 1.0 g (children, 25 mg/kg) IM or IV within 30 minutes before procedure.
Prophylactic Regimens for Genitourinary/Gastrointestinal Procedures. Total children’s dose should not exceed adult dose.
I.High-risk patients:
Ampicillin plus gentamicin: Ampicillin (adults, 2.0g; children, 50 mg/kg) plus gentamicin 1.5 mg/kg (for both adults and children, not to exceed 120 mg) IM or IV within 30 minutes before starting procedure. 6 hours later, ampicillin (adults, 1 g; children, 25 mg/kg) IM or IV, or amoxicillin (adults, 1.0g; children 25 mg/kg) orally.
II.High-risk patients allergic to ampicillin/amoxicillin:
Vancomycin plus gentamicin: Vancomycin (adults, 1.0g; children 20mg/kg) IV over 1-2 hours plus gentamicin 1.5 mg/kg (for both adults and children, not to exceed 120 mg) IM or IV. Complete injection/infusion within 30 minutes before starting procedure.
III.Moderate-risk patients:
Amoxicillin: Adults, 2.0 g (children 50 mg/kg) orally one hour before procedure.
-OR-
Ampicillin: Adults, 2.0 g (children, 50 mg/kg) IM or IV within 30 minutes before starting procedure.
IV.Moderate-risk patients allergic to ampicillin/amoxicillin:
Vancomycin: Adults, 1.0 g (children, 20 mg/kg) over 1-2 hours. Complete infusion within 30 minutes of starting the procedure.
Incorrect
Correct answer is D:
Secundum atrial septal defect does not require prophylaxis for subacute bacterial endocarditis.
Conditions for which endocarditis prophylaxis is recommended
High-risk category
•Prosthetic cardiac valves, including bioprosthetic and homograft valves
•Previous bacterial endocarditis
•Complex cyanotic congenital heart disease (e.g. single ventricle states, transposition of the great arteries, tetralogy of Fallot)
•Surgically constructed systemic to pulmonary shunts or conduits
Moderate-risk category
•Most other congenital cardiac malformations such as: patent ductus arteriosus, ventricular septal defect, primum atrial septal defect, coarctation of the aorta and bicuspid aortic valve.
•Mitral valve prolapse with valvar regurgitation and/or thickened leaflets
Conditions for which endocarditis prophylaxis is not recommended
Negligible-risk category (no greater risk than the general population)
•Isolated secundum atrial septal defect
•Surgical repair of atrial septal defect, ventricular septal defect, or patent ductus arteriosus (without residua beyond 6 months)
•Previous coronary artery bypass graft surgery
•Mitral valve prolapse without valvar regurgitation1
•Physiologic, functional, or innocent heart murmurs1
•Previous Kawasaki disease without valvar dysfunction
•Previous rheumatic fever without valvar dysfunction
•Cardiac pacemakers (intravascular and epicardial) and implanted defibrillators
Prophylactic Regimens for Dental, Oral, Respiratory Tract, or Esophageal Procedures (Follow-up dose no longer recommended.) Total children’s dose should not exceed adult dose.
A.Standard general prophylaxis for patients at risk:
Amoxicillin: Adults, 2.0g (children, 50 mg/kg) given orally one hour before procedure.
B.Unable to take oral medications:
Ampicillin: Adults 2.0 g (children, 50 mg/kg) given IM or IV within 30 minutes before procedure.
Clindamycin: Adults, 600 mg (children 20 mg/kg) orally one hour before procedure.
-OR-
Cephalexin or Cefadroxil: Adults 2.0 g (children 50 mg/kg) orally one hour before procedure. (Cephalosporins should not be used in patients with immediate-type hypersensitivity reaction to penicillin).
-OR-
Azithromycin or Clarithromycin: Adults, 500mg (children, 15 mg/kg) orally one hour before procedure.
D.Amoxicillin/ampicillin/penicillin-allergic patients unable to take oral medications:
Clindamycin: Adults, 600 mg (children, 20 mg/kg) IV within 30 minutes before procedure.
-OR-
Cefazolin: Adults 1.0 g (children, 25 mg/kg) IM or IV within 30 minutes before procedure.
Prophylactic Regimens for Genitourinary/Gastrointestinal Procedures. Total children’s dose should not exceed adult dose.
I.High-risk patients:
Ampicillin plus gentamicin: Ampicillin (adults, 2.0g; children, 50 mg/kg) plus gentamicin 1.5 mg/kg (for both adults and children, not to exceed 120 mg) IM or IV within 30 minutes before starting procedure. 6 hours later, ampicillin (adults, 1 g; children, 25 mg/kg) IM or IV, or amoxicillin (adults, 1.0g; children 25 mg/kg) orally.
II.High-risk patients allergic to ampicillin/amoxicillin:
Vancomycin plus gentamicin: Vancomycin (adults, 1.0g; children 20mg/kg) IV over 1-2 hours plus gentamicin 1.5 mg/kg (for both adults and children, not to exceed 120 mg) IM or IV. Complete injection/infusion within 30 minutes before starting procedure.
III.Moderate-risk patients:
Amoxicillin: Adults, 2.0 g (children 50 mg/kg) orally one hour before procedure.
-OR-
Ampicillin: Adults, 2.0 g (children, 50 mg/kg) IM or IV within 30 minutes before starting procedure.
IV.Moderate-risk patients allergic to ampicillin/amoxicillin:
Vancomycin: Adults, 1.0 g (children, 20 mg/kg) over 1-2 hours. Complete infusion within 30 minutes of starting the procedure.
Question 12 of 21
12. Question
1 points
Category: Acquired heart disease in children
Sub-acute bacterial endocarditis
A 3 year old who underwent surgical closure of secundum atrial septal defect 3 months ago will be undergoing a dental procedure. Child is active with no easy fatigability, shortness of breath or cyanosis. HR 100 beats per minute, respiratory rate 25 per minute, oxygen saturation is 99%. Physical examination is within normal limits.
Which of the following recommendations is correct regarding subacute bacterial endocarditis management?
Correct
That is Correct!
Secundum atrial septal defect does not require prophylaxis for subacute bacterial endocarditis, except for 6 months period after surgical or catheterization device closure.
Conditions for which endocarditis prophylaxis is recommended
High-risk category
•Prosthetic cardiac valves, including bioprosthetic and homograft valves
•Previous bacterial endocarditis
•Complex cyanotic congenital heart disease (e.g. single ventricle states, transposition of the great arteries, tetralogy of Fallot)
•Surgically constructed systemic to pulmonary shunts or conduits
Moderate-risk category
•Most other congenital cardiac malformations such as: patent ductus arteriosus, ventricular septal defect, primum atrial septal defect, coarctation of the aorta and bicuspid aortic valve.
•Mitral valve prolapse with valvar regurgitation and/or thickened leaflets
Conditions for which endocarditis prophylaxis is not recommended
Negligible-risk category (no greater risk than the general population)
•Isolated secundum atrial septal defect
•Surgical repair of atrial septal defect, ventricular septal defect, or patent ductus arteriosus (without residua beyond 6 months)
•Previous coronary artery bypass graft surgery
•Mitral valve prolapse without valvar regurgitation1
•Physiologic, functional, or innocent heart murmurs1
•Previous Kawasaki disease without valvar dysfunction
•Previous rheumatic fever without valvar dysfunction
•Cardiac pacemakers (intravascular and epicardial) and implanted defibrillators
Prophylactic Regimens for Dental, Oral, Respiratory Tract, or Esophageal Procedures (Follow-up dose no longer recommended.) Total children’s dose should not exceed adult dose.
A.Standard general prophylaxis for patients at risk:
Amoxicillin: Adults, 2.0g (children, 50 mg/kg) given orally one hour before procedure.
B.Unable to take oral medications:
Ampicillin: Adults 2.0 g (children, 50 mg/kg) given IM or IV within 30 minutes before procedure.
Clindamycin: Adults, 600 mg (children 20 mg/kg) orally one hour before procedure.
-OR-
Cephalexin or Cefadroxil: Adults 2.0 g (children 50 mg/kg) orally one hour before procedure. (Cephalosporins should not be used in patients with immediate-type hypersensitivity reaction to penicillin).
-OR-
Azithromycin or Clarithromycin: Adults, 500mg (children, 15 mg/kg) orally one hour before procedure.
D.Amoxicillin/ampicillin/penicillin-allergic patients unable to take oral medications:
Clindamycin: Adults, 600 mg (children, 20 mg/kg) IV within 30 minutes before procedure.
-OR-
Cefazolin: Adults 1.0 g (children, 25 mg/kg) IM or IV within 30 minutes before procedure.
Prophylactic Regimens for Genitourinary/Gastrointestinal Procedures. Total children’s dose should not exceed adult dose.
I.High-risk patients:
Ampicillin plus gentamicin: Ampicillin (adults, 2.0g; children, 50 mg/kg) plus gentamicin 1.5 mg/kg (for both adults and children, not to exceed 120 mg) IM or IV within 30 minutes before starting procedure. 6 hours later, ampicillin (adults, 1 g; children, 25 mg/kg) IM or IV, or amoxicillin (adults, 1.0g; children 25 mg/kg) orally.
II.High-risk patients allergic to ampicillin/amoxicillin:
Vancomycin plus gentamicin: Vancomycin (adults, 1.0g; children 20mg/kg) IV over 1-2 hours plus gentamicin 1.5 mg/kg (for both adults and children, not to exceed 120 mg) IM or IV. Complete injection/infusion within 30 minutes before starting procedure.
III.Moderate-risk patients:
Amoxicillin: Adults, 2.0 g (children 50 mg/kg) orally one hour before procedure.
-OR-
Ampicillin: Adults, 2.0 g (children, 50 mg/kg) IM or IV within 30 minutes before starting procedure.
IV.Moderate-risk patients allergic to ampicillin/amoxicillin:
Vancomycin: Adults, 1.0 g (children, 20 mg/kg) over 1-2 hours. Complete infusion within 30 minutes of starting the procedure.
Incorrect
Correct answer is A:
Secundum atrial septal defect does not require prophylaxis for subacute bacterial endocarditis, except for 6 months period after surgical or catheterization device closure.
Conditions for which endocarditis prophylaxis is recommended
High-risk category
•Prosthetic cardiac valves, including bioprosthetic and homograft valves
•Previous bacterial endocarditis
•Complex cyanotic congenital heart disease (e.g. single ventricle states, transposition of the great arteries, tetralogy of Fallot)
•Surgically constructed systemic to pulmonary shunts or conduits
Moderate-risk category
•Most other congenital cardiac malformations such as: patent ductus arteriosus, ventricular septal defect, primum atrial septal defect, coarctation of the aorta and bicuspid aortic valve.
•Mitral valve prolapse with valvar regurgitation and/or thickened leaflets
Conditions for which endocarditis prophylaxis is not recommended
Negligible-risk category (no greater risk than the general population)
•Isolated secundum atrial septal defect
•Surgical repair of atrial septal defect, ventricular septal defect, or patent ductus arteriosus (without residua beyond 6 months)
•Previous coronary artery bypass graft surgery
•Mitral valve prolapse without valvar regurgitation1
•Physiologic, functional, or innocent heart murmurs1
•Previous Kawasaki disease without valvar dysfunction
•Previous rheumatic fever without valvar dysfunction
•Cardiac pacemakers (intravascular and epicardial) and implanted defibrillators
Prophylactic Regimens for Dental, Oral, Respiratory Tract, or Esophageal Procedures (Follow-up dose no longer recommended.) Total children’s dose should not exceed adult dose.
A.Standard general prophylaxis for patients at risk:
Amoxicillin: Adults, 2.0g (children, 50 mg/kg) given orally one hour before procedure.
B.Unable to take oral medications:
Ampicillin: Adults 2.0 g (children, 50 mg/kg) given IM or IV within 30 minutes before procedure.
Clindamycin: Adults, 600 mg (children 20 mg/kg) orally one hour before procedure.
-OR-
Cephalexin or Cefadroxil: Adults 2.0 g (children 50 mg/kg) orally one hour before procedure. (Cephalosporins should not be used in patients with immediate-type hypersensitivity reaction to penicillin).
-OR-
Azithromycin or Clarithromycin: Adults, 500mg (children, 15 mg/kg) orally one hour before procedure.
D.Amoxicillin/ampicillin/penicillin-allergic patients unable to take oral medications:
Clindamycin: Adults, 600 mg (children, 20 mg/kg) IV within 30 minutes before procedure.
-OR-
Cefazolin: Adults 1.0 g (children, 25 mg/kg) IM or IV within 30 minutes before procedure.
Prophylactic Regimens for Genitourinary/Gastrointestinal Procedures. Total children’s dose should not exceed adult dose.
I.High-risk patients:
Ampicillin plus gentamicin: Ampicillin (adults, 2.0g; children, 50 mg/kg) plus gentamicin 1.5 mg/kg (for both adults and children, not to exceed 120 mg) IM or IV within 30 minutes before starting procedure. 6 hours later, ampicillin (adults, 1 g; children, 25 mg/kg) IM or IV, or amoxicillin (adults, 1.0g; children 25 mg/kg) orally.
II.High-risk patients allergic to ampicillin/amoxicillin:
Vancomycin plus gentamicin: Vancomycin (adults, 1.0g; children 20mg/kg) IV over 1-2 hours plus gentamicin 1.5 mg/kg (for both adults and children, not to exceed 120 mg) IM or IV. Complete injection/infusion within 30 minutes before starting procedure.
III.Moderate-risk patients:
Amoxicillin: Adults, 2.0 g (children 50 mg/kg) orally one hour before procedure.
-OR-
Ampicillin: Adults, 2.0 g (children, 50 mg/kg) IM or IV within 30 minutes before starting procedure.
IV.Moderate-risk patients allergic to ampicillin/amoxicillin:
Vancomycin: Adults, 1.0 g (children, 20 mg/kg) over 1-2 hours. Complete infusion within 30 minutes of starting the procedure.
Question 13 of 21
13. Question
1 points
Category: Pediatric cardiology pharmacology
Digoxin
The use of digoxin is contraindicated in all the following cases except one. Choose the condition from those listed below where digoxin is helpful.
Correct
That is correct!
Digoxin inhibits the sodium-potassium pump at the cellular membrane of cardiac tissue, causing increase intracellular levels of calcium. This will improve contractility and slows conduction. Therefore digoxin is useful in patients with heart failure and those requiring slowing of atrioventricular node conduction such as in Supraventricular tachycardia. Digoxin will worsen obstruction of patients with hypertrophic cardiomyopathy and may cause deterioration of ventricular arrhythmias. Digoxin is excreted predominantly through the kidneys, renal failure may be a contraindication to its use, however liver failure is not.
Incorrect
Correct answer is A:
Digoxin inhibits the sodium-potassium pump at the cellular membrane of cardiac tissue, causing increase intracellular levels of calcium. This will improve contractility and slows conduction. Therefore digoxin is useful in patients with heart failure and those requiring slowing of atrioventricular node conduction such as in Supraventricular tachycardia. Digoxin will worsen obstruction of patients with hypertrophic cardiomyopathy and may cause deterioration of ventricular arrhythmias. Digoxin is excreted predominantly through the kidneys, renal failure may be a contraindication to its use, however liver failure is not.
Question 14 of 21
14. Question
1 points
Category: Pediatric cardiology pharmacology
Diuretics
A 6 month old infant is recovering from surgical closure of ventricular septal defect. Furosemide is used as a diuretic to increase fluid output. The urine output was noted to decline over the past 2 days. Serum electrolytes are: sodium 137 mEq/L, Chloride 92 mEq/L, potassium 2.2 mEq/L, bicarbonate 50 mEq/L. Which of the following measures will help increase urine output?
Correct
That is Correct!
Furosemide is a loop diuretic which prevents reabsorbtion of chloride at the ascending loop of Henle in the kidneys. This will result in water wasting. Low serum chloride will minimize chloride reabsorbtion block in the ascending loop of Henle resulting in a reduced effect of diuresis. Therefore, correction of level of serum chloride through administration of potassium or ammonium chloride is needed. A higher dose of furosemide or adding another loop diuretic, such as bumetanide will have limited effect.
Incorrect
Correct answer is A:
Furosemide is a loop diuretic which prevents reabsorbtion of chloride at the ascending loop of Henle in the kidneys. This will result in water wasting. Low serum chloride will minimize chloride reabsorbtion block in the ascending loop of Henle resulting in a reduced effect of diuresis. Therefore, correction of level of serum chloride through administration of potassium or ammonium chloride is needed. A higher dose of furosemide or adding another loop diuretic, such as bumetanide will have limited effect.
Question 15 of 21
15. Question
1 points
Category: Pediatric cardiology pharmacology
Diuretics
A 2 month old with congestive heart failure secondary to double outlet right ventricle treated with digoxin, furosemide and spironolactone. If captopril is to be administered, what other changes are typically undertaken?
Correct
That is Correct!
Captopril and spironolactone both exert a potassium sparing effect on the kidneys, resulting in high serum potassium levels. Therefore, it is best to avoid using both medications simultaneously. Spironolactone is a weak diuretic and its use is mainly to counter the potassium wasting effect of furosemide.
Incorrect
Correct answer is B:
Captopril and spironolactone both exert a potassium sparing effect on the kidneys, resulting in high serum potassium levels. Therefore, it is best to avoid using both medications simultaneously. Spironolactone is a weak diuretic and its use is mainly to counter the potassium wasting effect of furosemide.
Question 16 of 21
16. Question
1 points
Category: Pediatric cardiology pharmacology
Captopril
A 6 year old boy with moderate mitral regurgitation secondary to rheumatic heart disease complains of recent onset dry cough. There is no history of fever or shortness of breath. Physical examination is within normal limits except for the holosystolic murmur at the cardiac apex. Lungs were clear to auscultation. The child has been treated with digoxin and lasix for the past 2 years. The doses of digoxin and lasix were increased recently to accommodate for weight gain and captopril was started because of increase mitral regurgitation in a recent echocardiogram. Chest x-ray shows cardiomegaly and prominent vascular markings.
Which of the following factors is the likely cause of cough in this child?
Correct
That is Correct!
This child is unlikely to have pneumonia in view of lack of fever and the dry nature of the cough. Chest x-ray shows increase vascular markings, probably due to dilated left atrium as a result of mitral regurgitation.
ACE inhibitors are known to cause dry cough, a brief period of withholding medication will clear the cough. This will assist in confirming the diagnosis.
Digoxin toxicity may result in fatigue, headache, nausea, anorexia, neuralgias, blurred vision, and photophobia. Cough is not a known effect of digoxin.
High doses of lasix may cause hypocalcaemia, not hyperclacemia. Neither cause cough.
Incorrect
Correct answer is D:
This child is unlikely to have pneumonia in view of lack of fever and the dry nature of the cough. Chest x-ray shows increase vascular markings, probably due to dilated left atrium as a result of mitral regurgitation.
ACE inhibitors are known to cause dry cough, a brief period of withholding medication will clear the cough. This will assist in confirming the diagnosis.
Digoxin toxicity may result in fatigue, headache, nausea, anorexia, neuralgias, blurred vision, and photophobia. Cough is not a known effect of digoxin.
High doses of lasix may cause hypocalcaemia, not hyperclacemia. Neither cause cough.
Question 17 of 21
17. Question
1 points
Category: Pediatric cardiology pharmacology
Captopril
Captopril, and ACE inhibitor, is beneficial to children with congestive heart failure secondary to large ventricular septal defect. Which of the following statements is correct regarding the mechanism through which captopril improves congestive heart failure in children with congestive heart failure secondary to left to right shunt lesions?
Correct
That is Correct!
Captopril assists in congestive heart failure by reducing systemic vascular resistance more than pulmonary vascular resistance; this will result in reducing the afterload encountered by the left ventricle and reduction of the volume of left to right shunt at the ventricular septal defect.
Incorrect
Correct answer is A:
Captopril assists in congestive heart failure by reducing systemic vascular resistance more than pulmonary vascular resistance; this will result in reducing the afterload encountered by the left ventricle and reduction of the volume of left to right shunt at the ventricular septal defect.
Question 18 of 21
18. Question
1 points
Category: Pediatric cardiology pharmacology
Aspirin
A 2 year old with girl with recent onset Kawasaki was treated with intravenous immunoglobulin infusion and acetyl salicylic acid 20 mg/kg/day. Echocardiography shows dilated proximal right and left main coronary arteries. Fever subsided and platelet count and erythrocyte sedimentation rate returned to normal values. Which of the following measures should be performed in view of the abnormal coronary arteries?
Correct
That is Correct!
Acetyl salicylic acid is initially used in the treatment of Kawasaki disease as an anti-inflammatory agent, once indicators of inflammation subside, such as fever; elevated platelet count, erythrocyte sedimentation rate then the dose could be reduced to an anti-platelet dose to prevent clot formation in the abnormal coronary arteries.
Incorrect
Correct answer is C:
Acetyl salicylic acid is initially used in the treatment of Kawasaki disease as an anti-inflammatory agent, once indicators of inflammation subside, such as fever; elevated platelet count, erythrocyte sedimentation rate then the dose could be reduced to an anti-platelet dose to prevent clot formation in the abnormal coronary arteries.
Question 19 of 21
19. Question
1 points
Category: Pediatric cardiology pharmacology
Aspirin
Anticoagulation effect of acetyl salicylic acid is achieved through which one of the following mechanisms?
Correct
That is Correct!
Item A is the mode of action of heparin.
Item B is the mode of action of warfarin.
Item C is the mode of action of enoxaparin.
Incorrect
Correct answer is D:
Item A is the mode of action of heparin.
Item B is the mode of action of warfarin.
Item C is the mode of action of enoxaparin.
Question 20 of 21
20. Question
1 points
Category: Pediatric cardiology pharmacology
Beta blockers
Patients with cardio-neurogenic syncope benefit from beta-blockers. What is the method of action through which these agents prevent syncope?
Correct
That is Correct!
When standing up, the systemic venous return from the lower extremities is reduced. This is further exaggerated if the individual is dehydrated, such as early in the morning and after sports. The reduced venous blood to the heart triggers increase contractility of the ventricles to compensate for the reduced cardiac output. This forceful contraction inadvertently stimulates in some individuals the C-fibers which are typically stimulated through stretching in cases of hypertension and increased intravascular volume. When the C-fibers are stimulated, bradycardia develops, which further reduces cardiac output, causing syncope.
Beta-blockers disrupts this cycle through its negative inotropic effect, preventing forceful contraction of the ventricles, thus preventing stimulation of the C-fibers.
Patients with cardio-neurogenic syncope typically develop bradycardia and not tachycardia. Blood pressure drops in such patients as well. Beta-blockers cause bronchoconstriction and air movement is not an issue in cardio-neurogenic syncope.
Incorrect
Correct answer is B:
When standing up, the systemic venous return from the lower extremities is reduced. This is further exaggerated if the individual is dehydrated, such as early in the morning and after sports. The reduced venous blood to the heart triggers increase contractility of the ventricles to compensate for the reduced cardiac output. This forceful contraction inadvertently stimulates in some individuals the C-fibers which are typically stimulated through stretching in cases of hypertension and increased intravascular volume. When the C-fibers are stimulated, bradycardia develops, which further reduces cardiac output, causing syncope.
Beta-blockers disrupts this cycle through its negative inotropic effect, preventing forceful contraction of the ventricles, thus preventing stimulation of the C-fibers.
Patients with cardio-neurogenic syncope typically develop bradycardia and not tachycardia. Blood pressure drops in such patients as well. Beta-blockers cause bronchoconstriction and air movement is not an issue in cardio-neurogenic syncope.
Question 21 of 21
21. Question
1 points
Category: Pediatric cardiology pharmacology
Beta blockers
A 5 year old boy presents with palpitation of 1-2 days duration. Other than rapid heart rate the physical examination is within normal limits. The child is not known to have congenital heart disease. Of the following medications, which agent/maneuver may be able to convert this rhythm to normal sinus rhythm?
m10
m10
Correct
That is Correct!
This child has atrial flutter, caused by an abnormal circuit of cells within the atrial tissue causing tachyarrhythmia. This child has 4:1 or 5:1 atrioventricular block. Beta-blockers can cause abolition of arrhythmias within the atrial or ventricular tissue. Agents which slow the atrioventricular nodal conduction (such as adenosine or Valsalva maneuver) will not abolish this arrhythmia, though they may slow the atrio-ventricular conduction. Lidocain affects ventricular tissue and has no effect on atrial tissue.
Incorrect
Correct answer is A:
This child has atrial flutter, caused by an abnormal circuit of cells within the atrial tissue causing tachyarrhythmia. This child has 4:1 or 5:1 atrioventricular block. Beta-blockers can cause abolition of arrhythmias within the atrial or ventricular tissue. Agents which slow the atrioventricular nodal conduction (such as adenosine or Valsalva maneuver) will not abolish this arrhythmia, though they may slow the atrio-ventricular conduction. Lidocain affects ventricular tissue and has no effect on atrial tissue.